

Reductions in 28-day mortality following hospital admission for upper gastrointestinal hemorrhage
- PMID: 21447331
- PMCID: PMC3194090
- DOI: 10.1053/j.gastro.2011.03.048
Reductions in 28-day mortality following hospital admission for upper gastrointestinal hemorrhage
Abstract
Background & aims: It is unclear whether mortality from upper gastrointestinal hemorrhage is changing: any differences observed might result from changes in age or comorbidity of patient populations. We estimated trends in 28-day mortality in England following hospital admission for gastrointestinal hemorrhage.
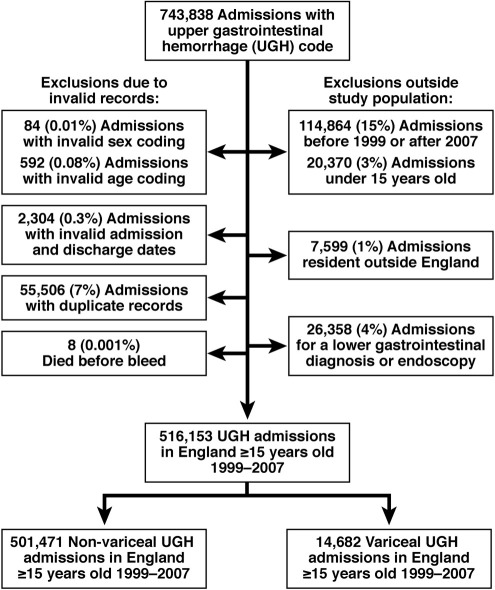
Methods: We used a case-control study design to analyze data from all adults administered to a National Health Service hospital, for upper gastrointestinal hemorrhage, from 1999 to 2007 (n=516,153). Cases were deaths within 28 days of admission (n=74,992), and controls were survivors to 28 days. The 28-day mortality was derived from the linked national death register. A logistic regression model was used to adjust trends in nonvariceal and variceal hemorrhage mortality for age, sex, and comorbidities and to investigate potential interactions.
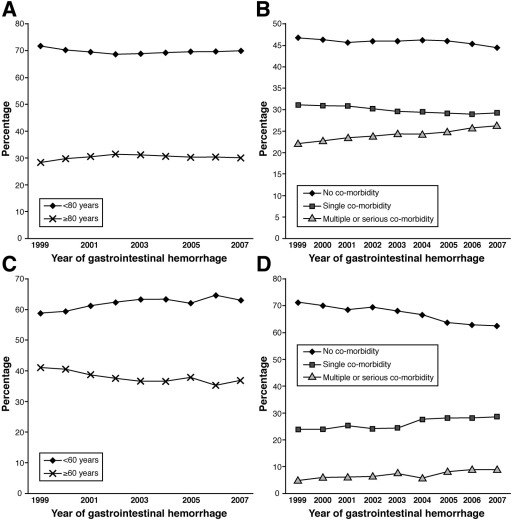
Results: During the study period, the unadjusted, overall, 28-day mortality following nonvariceal hemorrhage was reduced from 14.7% to 13.1% (unadjusted odds ratio, 0.87; 95% confidence interval: 0.84-0.90). The mortality following variceal hemorrhage was reduced from 24.6% to 20.9% (unadjusted odds ratio, 0.8; 95% confidence interval: 0.69-0.95). Adjustments for age and comorbidity partly accounted for the observed trends in mortality. Different mortality trends were identified for different age groups following nonvariceal hemorrhage.
Conclusions: The 28-day mortality in England following both nonvariceal and variceal upper gastrointestinal hemorrhage decreased from 1999 to 2007, and the reduction had been partly obscured by changes in patient age and comorbidities. Our findings indicate that the overall management of bleeding has improved within the first 4 weeks of admission.
Copyright © 2011 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lanas A., Garcia-Rodriguez L.A., Polo-Tomas M. Time trends and impact of upper and lower gastrointestinal bleeding and perforation in clinical practice. Am J Gastroenterol. 2009;104:1633–1641. - PubMed
-
- van Leerdam M.E., Vreeburg E.M., Rauws E.A.J. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol. 2003;98:1494–1499. - PubMed
-
- Targownik L.E., Nabalamba A. Trends in management and outcomes of acute nonvariceal upper gastrointestinal bleeding: 1993–2003. Clin Gastroenterol Hepatol. 2006;4:1459–1466. - PubMed
-
- Barkun A.N., Bardou M., Kuipers E.J. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2010;152:101–113. - PubMed
-
- Gralnek I.M., Barkun A.N., Bardou M. Management of acute bleeding from a peptic ulcer. N Engl J Med. 2008;359:928–937. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
