

Dynamic changes of edema and late gadolinium enhancement after acute myocardial infarction and their relationship to functional recovery and salvage index
- PMID: 21447711
- PMCID: PMC3098134
- DOI: 10.1161/CIRCIMAGING.111.963421
Dynamic changes of edema and late gadolinium enhancement after acute myocardial infarction and their relationship to functional recovery and salvage index
Abstract
Background: Changes in the myocardium in acute ischemia are dynamic and complex, and the characteristics of myocardial tissue on cardiovascular magnetic resonance in the acute setting are not fully defined. We investigated changes in edema and late gadolinium enhancement (LGE) with serial imaging early after acute myocardial infarction, relating these to global and segmental myocardial function at 6 months.
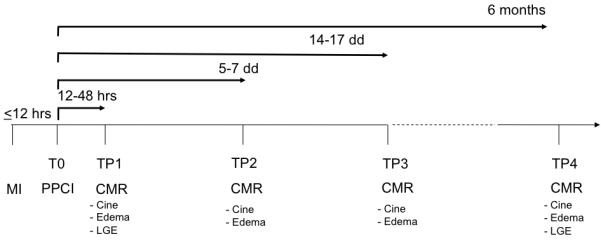
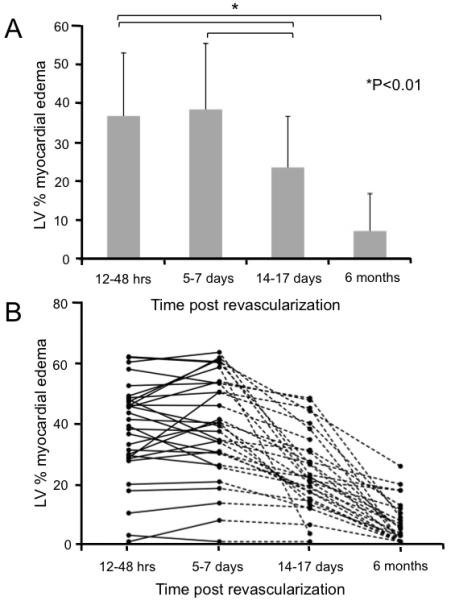
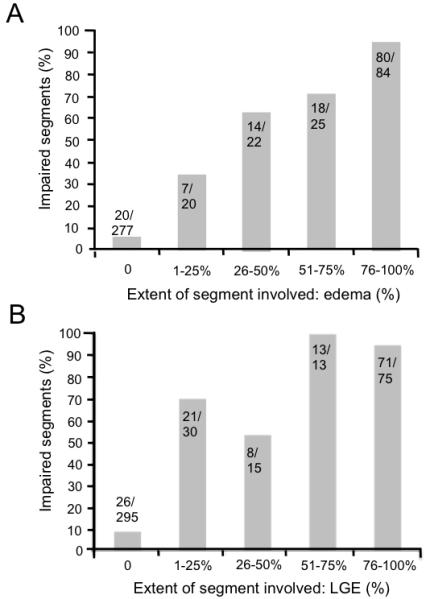
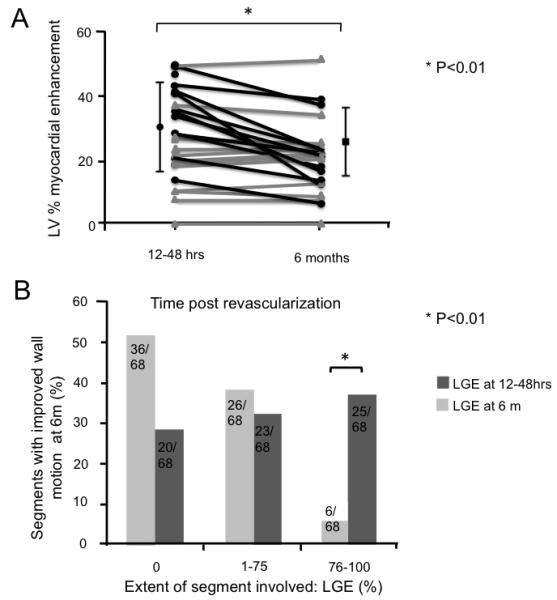
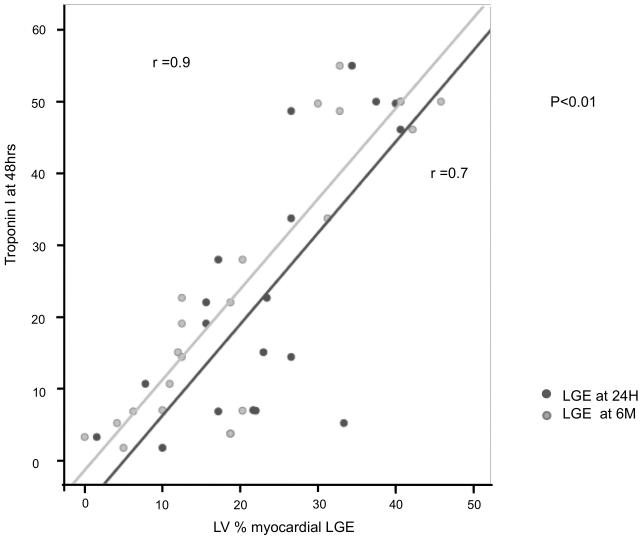
Methods and results: Cardiovascular magnetic resonance scans were performed on 30 patients with ST-elevation--myocardial infarction treated by primary percutaneous coronary intervention at each of 4 time points: 12 to 48 hours; 5 to 7 days; 14 to 17 days; and 6 months. All patients showed edema at 24 hours. The mean volume of edema (% left ventricle) was 37±16 at 24 hours and 39±17 at 1 week, with a reduction to 24±13 (P<0.01) by 2 weeks. Myocardial segments with edema also had increased signal on LGE at 24 hours (κ=0.77; P<0.001). The volume of LGE decreased significantly between 24 hours and 6 months (27±15% versus 22±12%; P=0.002). Of segments showing LGE at 24 hours, 50% showed resolution by 6 months. In segments with such a reduction in LGE, 65% also showed improved wall motion (P<0.0001). The area of LGE measured at 6 months correlated more strongly with troponin at 48 hours (r=0.9; P<0.01) than LGE at 24 hours (r=0.7). The difference in LGE between 24 hours and 6 months had profound effects on the calculation of salvage index (26±21% at 24 hours versus 42±23% at 6 months; P=0.02).
Conclusions: Myocardial edema is maximal and constant over the first week after myocardial infarction, providing a stable window for the retrospective evaluation of area at risk. By contrast, myocardial areas with high signal intensity in LGE images recede over time with corresponding recovery of function, indicating that acutely detected LGE does not necessarily equate with irreversible injury and may severely underestimate salvaged myocardium.
Figures

Comment in
-
T2-cardiac magnetic resonance: has Elvis left the building?Circ Cardiovasc Imaging. 2011 May;4(3):198-200. doi: 10.1161/CIRCIMAGING.111.965343. Circ Cardiovasc Imaging. 2011. PMID: 21586742 No abstract available.
References
-
- Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. - PubMed
-
- Aletras AH, Tilak GS, Natanzon A, Hsu L-Y, Gonzalez FM, Hoyt RF, Jr., Arai AE. Retrospective determination of the area at risk for reperfused acute myocardial infarction with t2-weighted cardiac magnetic resonance imaging: Histopathological and displacement encoding with stimulated echoes (dense) functional validations. Circulation. 2006;113:1865–1870. - PubMed
-
- Cury RC, Shash K, Nagurney JT, Rosito G, Shapiro MD, Nomura CH, Abbara S, Bamberg F, Ferencik M, Schmidt EJ, Brown DF, Hoffmann U, Brady TJ. Cardiac magnetic resonance with t2-weighted imaging improves detection of patients with acute coronary syndrome in the emergency department. Circulation. 2008;118:837–844. - PubMed
-
- Abdel-Aty H, Cocker M, Meek C, Tyberg JV, Friedrich MG. Edema as a very early marker for acute myocardial ischemia: A cardiovascular magnetic resonance study. J Am Coll Cardiol. 2009;53:1194–1201. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
