

Surgical technique: the anterosuperior approach for reverse shoulder arthroplasty
- PMID: 21448776
- PMCID: PMC3148356
- DOI: 10.1007/s11999-011-1861-7
Surgical technique: the anterosuperior approach for reverse shoulder arthroplasty
Abstract
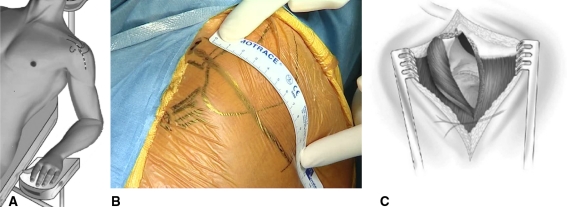
Background: The anterosuperior approach used for reverse shoulder arthroplasty is an intermediate between the transacromial approach originally proposed by Paul Grammont and the anterosuperior approach described by D. B. Mackenzie for shoulder arthroplasty. As an alternative to the deltopectoral approach, the anterosuperior approach has the advantages of simplicity and postoperative stability.
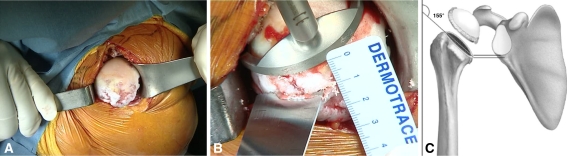
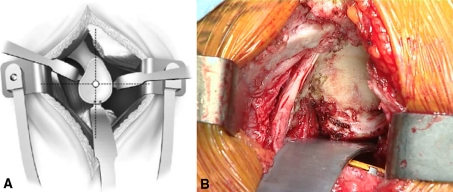
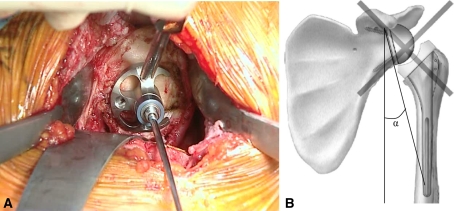
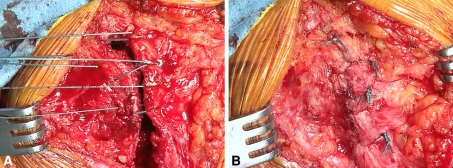
Description of technique: The anterior deltoid is divided from the anterior edge of the acromioclavicular arch, allowing exposure to the glenoid for glenosphere implantation.
Patients and methods: We used the findings of published studies to assess instability, function and pain scores, scapular notching, and complications after this approach.
Results: In a comparison of the deltopectoral and anterosuperior approaches in 527 reverse arthroplasties with a minimum 2-year followup, postoperative instability rate was greater with the deltopectoral (5.1%) than with the anterosuperior (0.8%) approach. Other published studies confirm this finding. No differences in Constant-Murley score or active mobility were found. Scapular notching occurred at similar rates after the anterosuperior (74%) and deltopectoral (63%) approaches. Humeral diaphyseal fracture rates were similar, whereas the acromial fracture rate was higher using the deltopectoral approach. Loosening tended to occur more often with the anterosuperior approach.
Conclusions: The anterosuperior approach can be used in primary and revision reverse shoulder arthroplasty, as well as in acute humeral head fracture. Its main apparent advantages are simplicity, ease of axial humerus preparation, quality of frontal exposure of the glenoid, and due to subscapularis tendon preservation, a low risk of postoperative instability. Its drawbacks are risk of inaccurate glenoid positioning, axillary nerve palsy, and deltoid weakening.
Figures
References
-
- Boileau P, Chuinard C, Roussanne Y, Bicknell RT, Rochet N, Trojani C. Reverse shoulder arthroplasty combined with a modified latissimus dorsi and teres major tendon transfer for shoulder pseudoparalysis associated with dropping arm. Clin Orthop Relat Res. 2008;466:584–593. doi: 10.1007/s11999-008-0114-x. - DOI - PMC - PubMed
-
- Bufquin T, Hersan A, Hubert L, Massin P. Reverse shoulder arthroplasty for the treatment of three- and four-part fractures of the proximal humerus in the elderly: a prospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br. 2007;89:516–520. doi: 10.1302/0301-620X.89B4.18435. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
