

Pulmonary tumor thrombotic microangiopathy induced by gastric carcinoma: morphometric and immunohistochemical analysis of six autopsy cases
- PMID: 21450103
- PMCID: PMC3072924
- DOI: 10.1186/1746-1596-6-27
Pulmonary tumor thrombotic microangiopathy induced by gastric carcinoma: morphometric and immunohistochemical analysis of six autopsy cases
Abstract
Background: Pulmonary tumor thrombotic microangiopathy (PTTM) has been known as a rare and serious cancer-related pulmonary complication. However, the pathogenesis and pathophysiology of this debilitating condition still remains obscure and no effective management was recommended. The present study aims to elucidate the pathophysiology of PTTM.
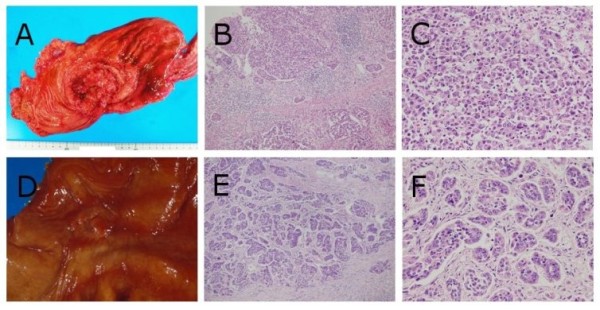
Methods: Autopsy records were searched to extract cases of pulmonary tumor embolism induced by metastasis of gastric carcinoma in the Toho University Omori Medical Center from 2000 to 2006. And then, tissue sections of extracted cases were prepared for not only light microscopic observation but morphometric analysis with the use of selected PTTM cases.
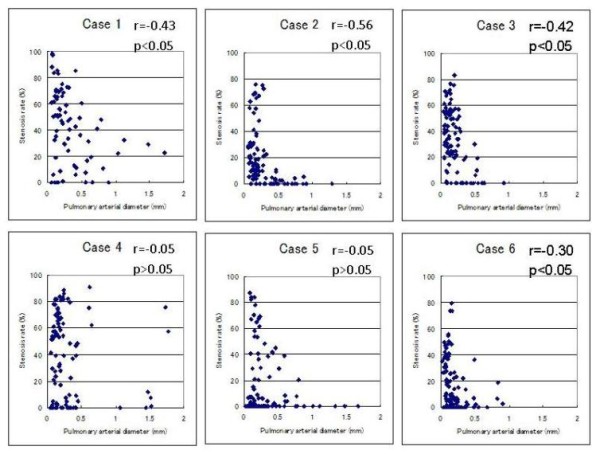
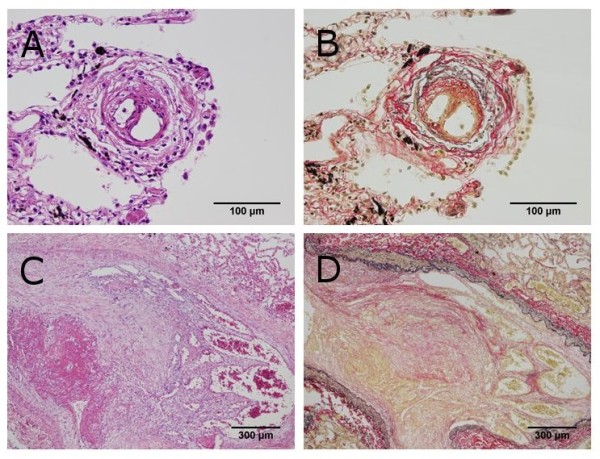
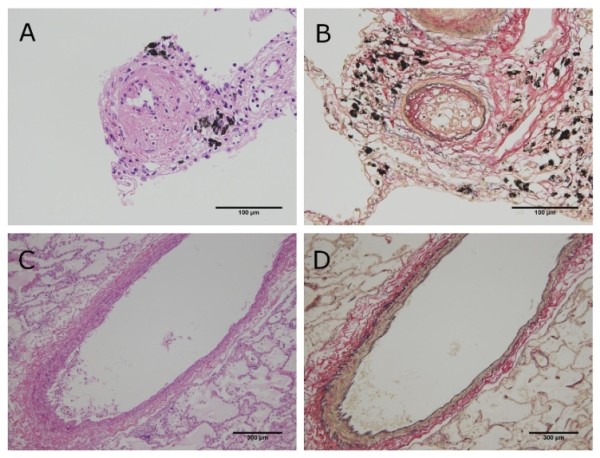
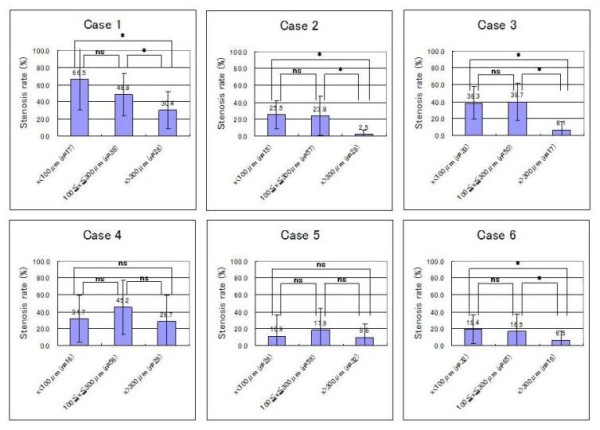
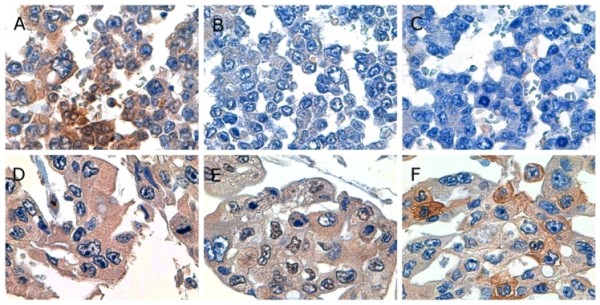
Results: Six autopsies involved PTTM and clinicopathological data of them were summarized. There was a significant negative association between pulmonary arterial diameter and stenosis rate in four cases. Although all cases showed an increase of stenosis rate to some degree, the degree of stenosis rate varied from case to case. Significant differences were found for average stenosis rate between the under 100 micrometer group or the 100 to 300 micrometer group and the 300 micrometer group in four cases. However, no significant differences were found for average stenosis rate between the under 100 micrometer group and the 100 to 300 micrometer group in all cases. Meanwhile, all cases showed positive reactivity for tissue factor (TF), five showed positive reactivity for vascular endothelial growth factor (VEGF), and three showed positive reactivity for osteopontin (OPN).
Conclusions: In the present study, we revealed that the degree of luminal narrowing of the pulmonary arteries varied from case to case, and our results suggested that pulmonary hypertension in PTTM occurs in selected cases which have a widespread pulmonary lesion with severe luminal narrowing in the smaller arteries. Furthermore, our immunohistochemical examination indicated that gastric carcinoma indicating PTTM shows a higher TF-positive rate than typical gastric carcinoma. However, it remains still obscuring whether gastric carcinoma indicating PTTM shows a higher VEGF or OPN-positive rate as determined by immunohistochemistry.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
