

Protective efficacy of co-trimoxazole prophylaxis against malaria in HIV exposed children in rural Uganda: a randomised clinical trial
- PMID: 21454456
- PMCID: PMC3068910
- DOI: 10.1136/bmj.d1617
Protective efficacy of co-trimoxazole prophylaxis against malaria in HIV exposed children in rural Uganda: a randomised clinical trial
Abstract
Objective: To evaluate the protective efficacy of co-trimoxazole prophylaxis against malaria in HIV exposed children (uninfected children born to HIV infected mothers) in Africa.
Design: Non-blinded randomised control trial
Setting: Tororo district, rural Uganda, an area of high malaria transmission intensity
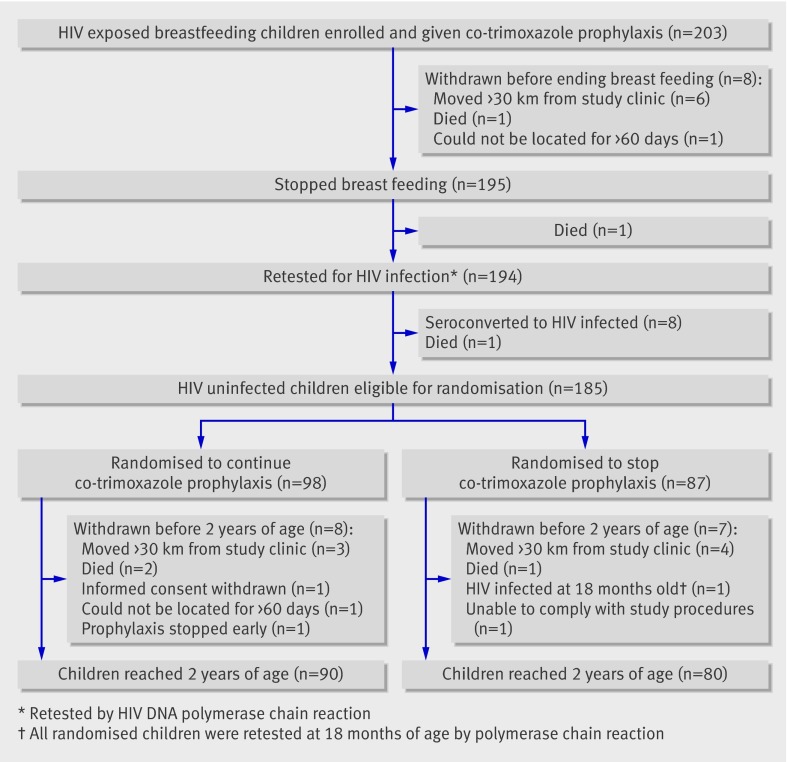
Participants: 203 breastfeeding HIV exposed infants enrolled between 6 weeks and 9 months of age
Intervention: Co-trimoxazole prophylaxis from enrollment until cessation of breast feeding and confirmation of negative HIV status. All children who remained HIV uninfected (n = 185) were then randomised to stop co-trimoxazole prophylaxis immediately or continue co-trimoxazole until 2 years old.
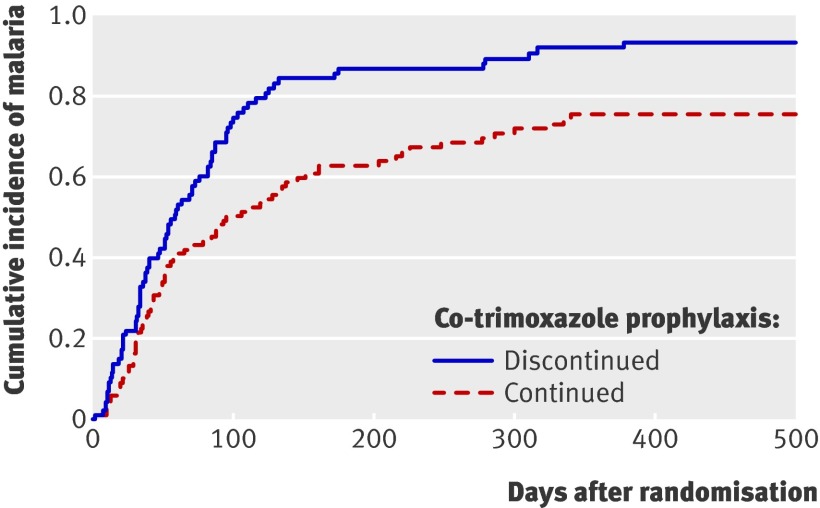
Main outcome measure: Incidence of malaria, calculated as the number of antimalarial treatments per person year.
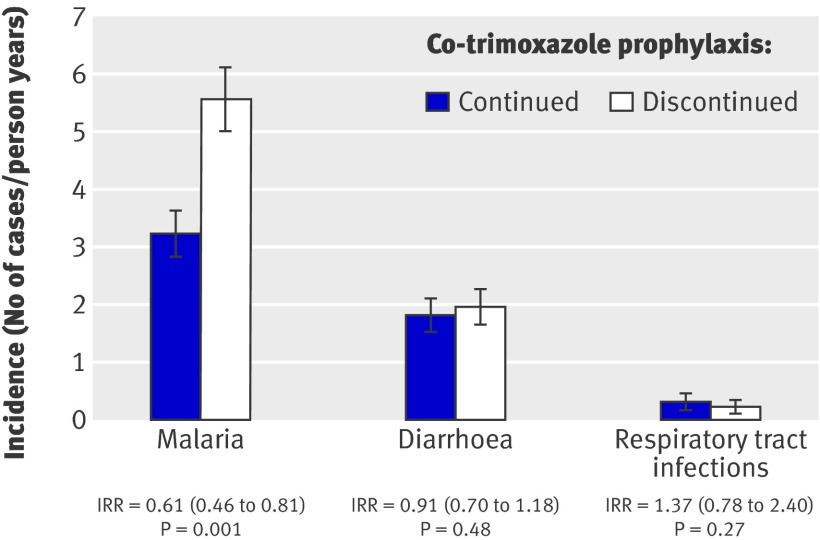
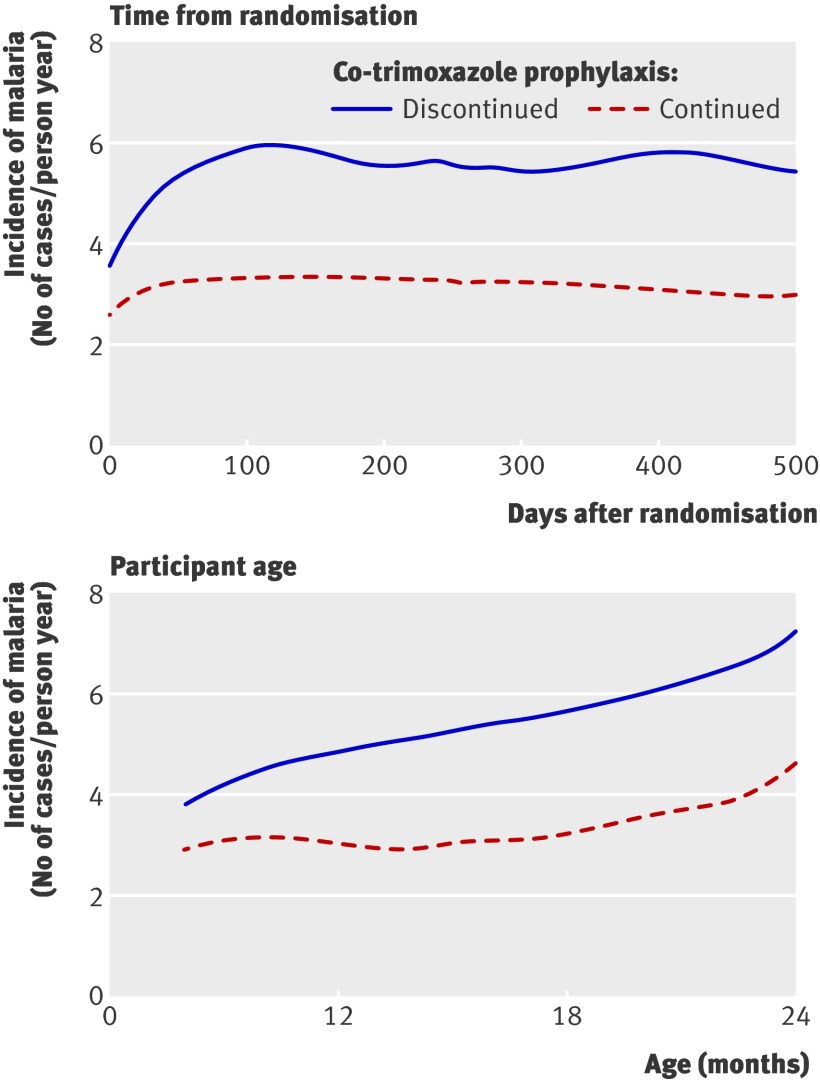
Results: The incidence of malaria and prevalence of genotypic mutations associated with antifolate resistance were high throughout the study. Among the 98 infants randomised to continue co-trimoxazole, 299 malaria cases occurred in 92.28 person years (incidence 3.24 cases/person year). Among the 87 infants randomised to stop co-trimoxazole, 400 malaria cases occurred in 71.81 person years (5.57 cases/person year). Co-trimoxazole prophylaxis yielded a 39% reduction in malaria incidence, after adjustment for age at randomisation (incidence rate ratio 0.61 (95% CI 0.46 to 0.81), P = 0.001). There were no significant differences in the incidence of complicated malaria, diarrhoea, pneumonia, hospitalisations, or deaths between the two treatment arms.
Conclusions: Co-trimoxazole prophylaxis was moderately protective against malaria in HIV exposed infants when continued beyond the period of HIV exposure despite the high prevalence of Plasmodium genotypes associated with antifolate resistance. Trial registration Clinical Trials NCT00527800.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- World Health Organization & Roll Back Malaria. Malaria and HIV interactions and their implications for public health policy. Report of a technical consultation, Geneva, Switzerland, 23-5 June 2004. 2010. www.who.int/hiv/pub/prev_care/malariahiv.pdf.
-
- Joint United Nations Programme on HIV/AIDS, (UNAIDS) & World Health Organization (WHO). AIDS epidemic update: November 2009. UNAIDS and WHO, 2009.
-
- Brahmbhatt H, Kigozi G, Wabwire-Mangen F, Serwadda D, Lutalo T, Nalugoda F, et al. Mortality in HIV-infected and uninfected children of HIV-infected and uninfected mothers in rural Uganda. J Acquir Immune Defic Syndr 2006;41:504-8. - PubMed
-
- Crampin AC, Floyd S, Glynn JR, Madise N, Nyondo A, Khondowe MM, et al. The long-term impact of HIV and orphanhood on the mortality and physical well-being of children in rural Malawi. Aids 2003;17:389-97. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical