

Preexisting statin use is associated with greater reperfusion in hyperacute ischemic stroke
- PMID: 21454815
- PMCID: PMC3125694
- DOI: 10.1161/STROKEAHA.110.600957
Preexisting statin use is associated with greater reperfusion in hyperacute ischemic stroke
Abstract
Background and purpose: Statin pretreatment has been associated with improved outcomes in patients with ischemic stroke. Although several mechanisms have been examined in animal models, few have been examined in patients. We hypothesized that patients using statins before stroke onset may have greater reperfusion than patients not using statins.
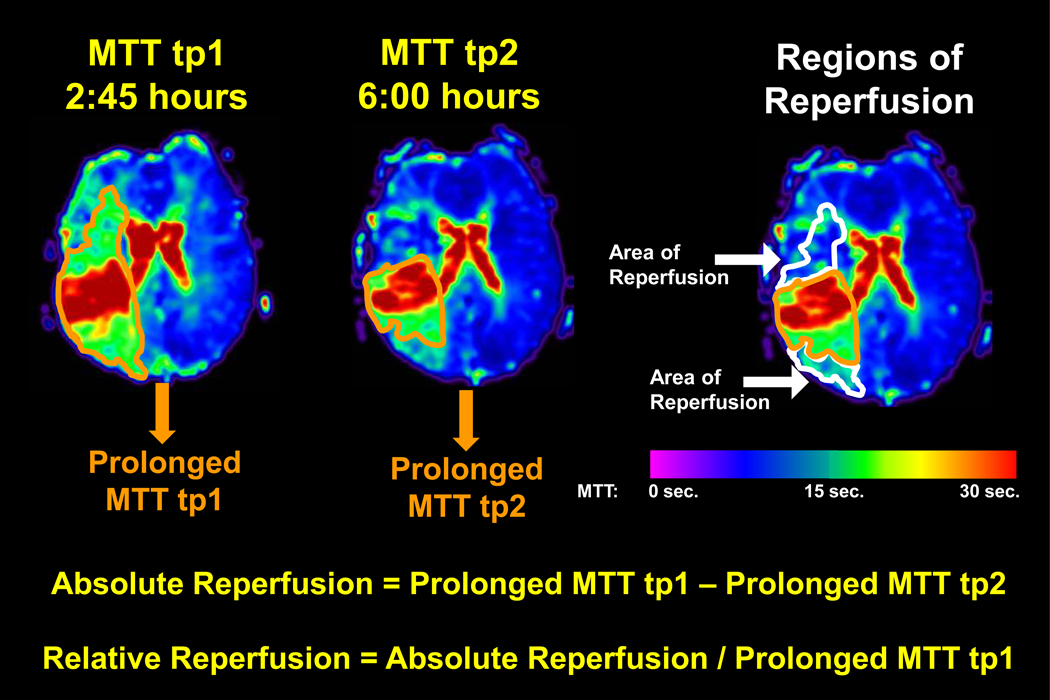
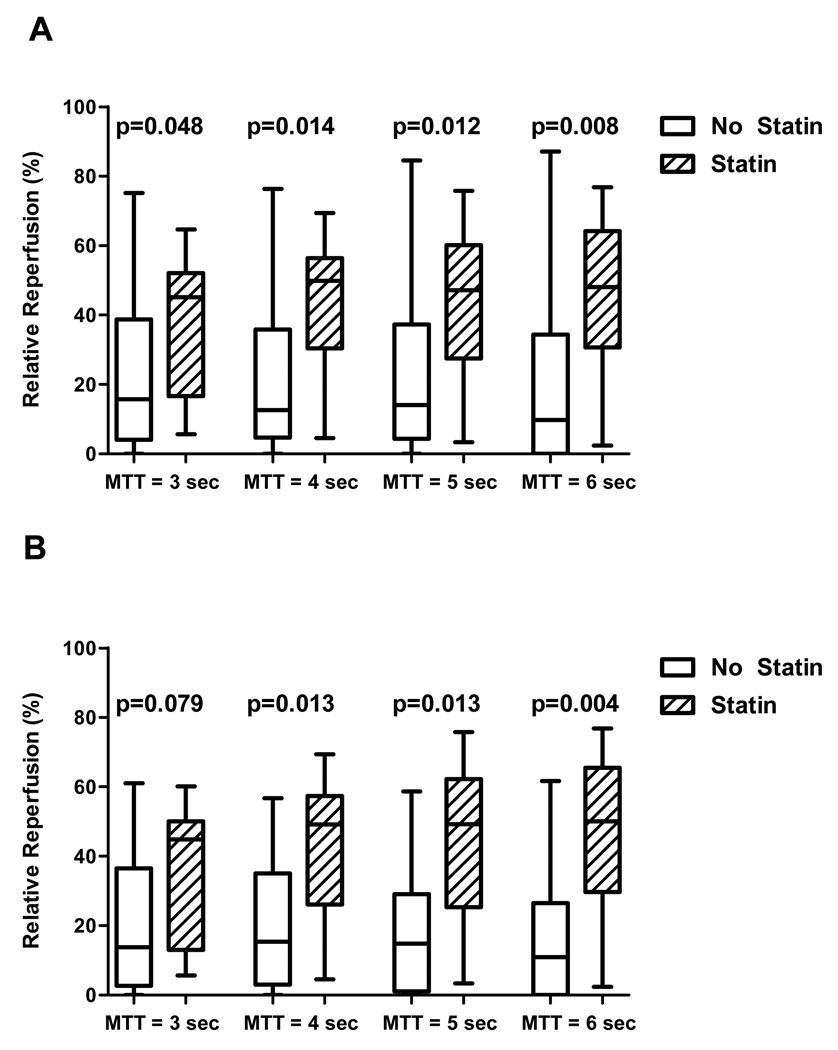
Methods: Acute ischemic stroke patients underwent 2 MR scans: within 4.5 (tp1) and at 6 hours (tp2) after stroke onset. Regions of reperfusion were defined by prolonged mean transit time (MTT) at tp1, which normalized at tp2. Four MTT thresholds were assessed to ensure that results were not spuriously based on an arbitrary threshold. Baseline characteristics, relative reperfusion, and change in NIHSS between tp1 and 1-month follow-up (ΔNIHSS) were compared between patients who were using statins at stroke onset and those who were not.
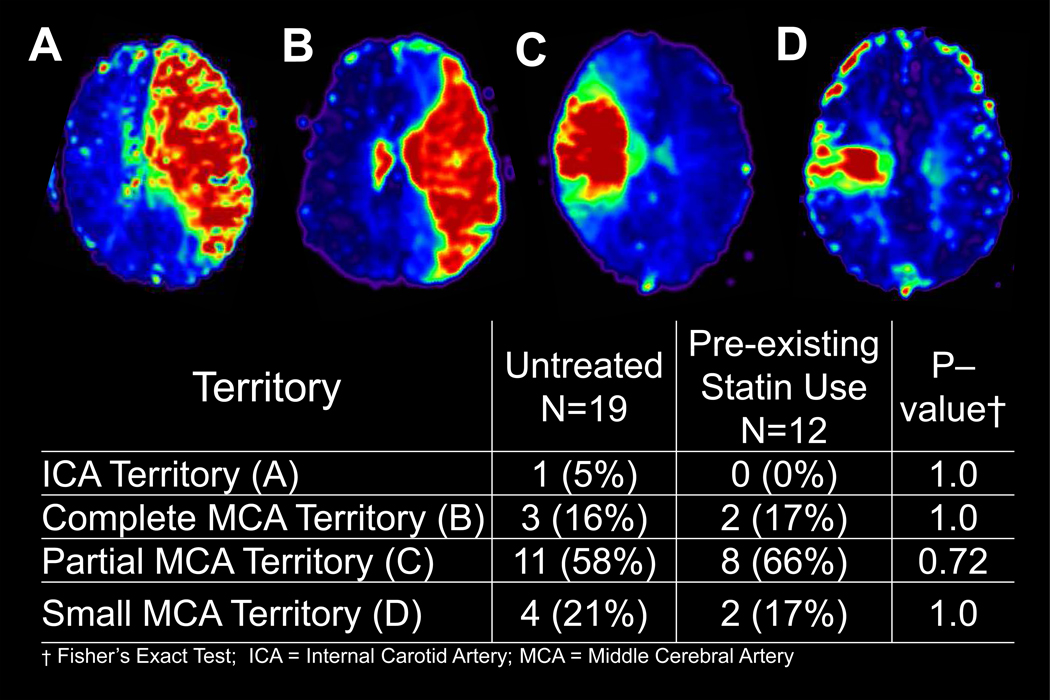
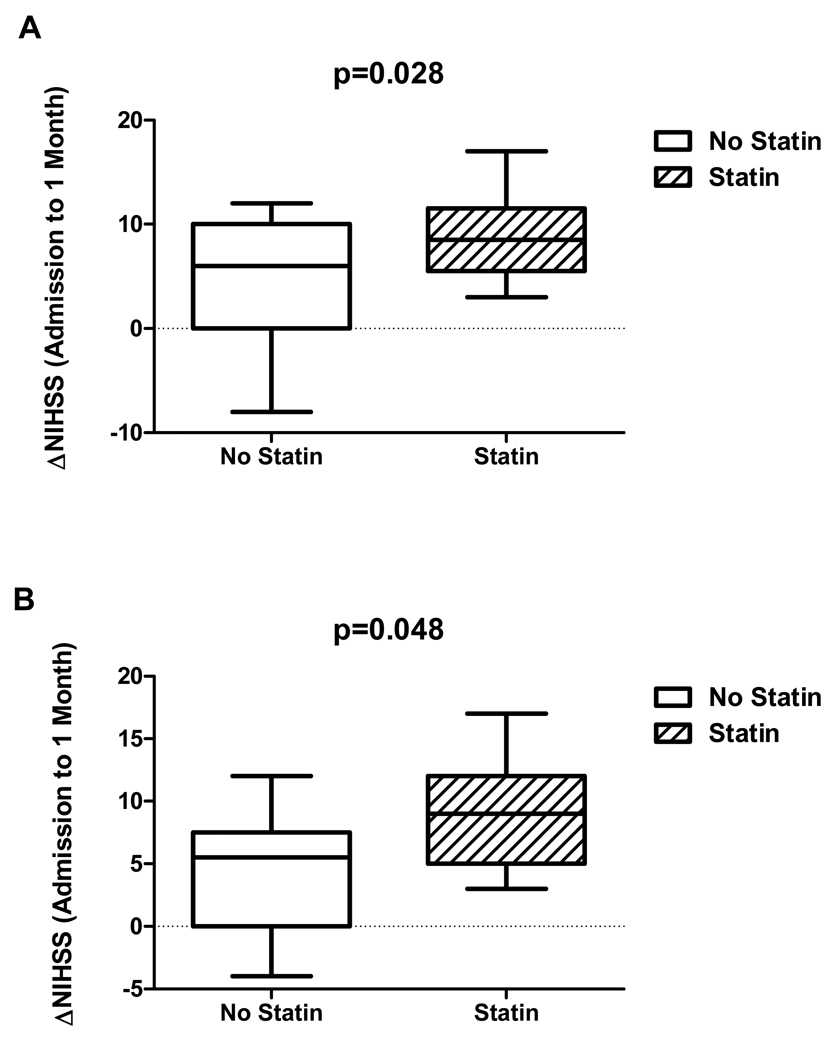
Results: Thirty-one stroke patients were prospectively enrolled; 12 were using statins and 19 were not. Baseline characteristics did not differ between the 2 groups except the statin group had greater coronary artery disease (P=0.03). Patients using statins showed significantly greater reperfusion compared to untreated patients across all MTT thresholds. For MTT of 4 seconds, median relative reperfusion was 50% (interquartile range, 30%-56%) in the preexisting statin group versus 13% (interquartile range, 5%-36%) in the untreated group (P=0.014). The statin group had greater ΔNIHSS (8.8±4.0 points) compared to the untreated group (4.4±5.7 points; P=0.028).
Conclusions: Statin use before ischemic stroke onset was associated with greater early reperfusion and NIHSS improvement. Further studies in larger populations are required to confirm our preliminary findings.
Figures
Similar articles
-
Clinically relevant reperfusion in acute ischemic stroke: MTT performs better than Tmax and TTP.Transl Stroke Res. 2014 Jun;5(3):415-421. doi: 10.1007/s12975-014-0325-2. Epub 2014 Feb 6. Transl Stroke Res. 2014. PMID: 24500786 Free PMC article.
-
Early changes of tissue perfusion after tissue plasminogen activator in hyperacute ischemic stroke.Stroke. 2011 Jan;42(1):65-72. doi: 10.1161/STROKEAHA.110.590323. Epub 2010 Dec 9. Stroke. 2011. PMID: 21148444 Free PMC article. Clinical Trial.
-
Statin therapy does not affect the radiographic and clinical profile of patients with TIA and minor stroke.AJNR Am J Neuroradiol. 2015 Jun;36(6):1076-80. doi: 10.3174/ajnr.A4257. Epub 2015 Apr 23. AJNR Am J Neuroradiol. 2015. PMID: 25907521 Free PMC article.
-
Statin treatment and functional outcome after ischemic stroke: case-control and meta-analysis.Stroke. 2011 May;42(5):1314-9. doi: 10.1161/STROKEAHA.110.605923. Epub 2011 Mar 17. Stroke. 2011. PMID: 21415396 Free PMC article. Review.
-
Statins for the Prevention of Post-Stroke Seizure and Epilepsy Development: A Systematic Review and Meta-Analysis.J Stroke Cerebrovasc Dis. 2021 Oct;30(10):106024. doi: 10.1016/j.jstrokecerebrovasdis.2021.106024. Epub 2021 Aug 23. J Stroke Cerebrovasc Dis. 2021. PMID: 34438280
Cited by
-
Transporter-Mediated Delivery of Small Molecule Drugs to the Brain: A Critical Mechanism That Can Advance Therapeutic Development for Ischemic Stroke.Pharmaceutics. 2020 Feb 14;12(2):154. doi: 10.3390/pharmaceutics12020154. Pharmaceutics. 2020. PMID: 32075088 Free PMC article. Review.
-
Effect of drug interventions on cerebral hemodynamics in ischemic stroke patients.J Cereb Blood Flow Metab. 2022 Mar;42(3):471-485. doi: 10.1177/0271678X211058261. Epub 2021 Nov 5. J Cereb Blood Flow Metab. 2022. PMID: 34738511 Free PMC article. Review.
-
Impact of pretreatment and early treatment with statins on safety and efficacy outcomes in patients after acute ischemic stroke undergoing endovascular thrombectomy: a systematic review and meta-analysis.Neuroradiology. 2025 Apr;67(4):995-1007. doi: 10.1007/s00234-025-03583-4. Epub 2025 Mar 25. Neuroradiology. 2025. PMID: 40131432
-
Statins in Neuro-ophthalmology.Neuroophthalmology. 2020 Jun 24;45(4):219-237. doi: 10.1080/01658107.2020.1755872. eCollection 2021. Neuroophthalmology. 2020. PMID: 34366510 Free PMC article. Review.
-
Reperfusion Beyond 6 Hours Reduces Infarct Probability in Moderately Ischemic Brain Tissue.Stroke. 2016 Jan;47(1):99-105. doi: 10.1161/STROKEAHA.115.010656. Epub 2015 Nov 19. Stroke. 2016. PMID: 26585394 Free PMC article.
References
-
- Amarenco P, Bogousslavsky J, Callahan A, 3rd, Goldstein LB, Hennerici M, Rudolph AE, Sillesen H, Simunovic L, Szarek M, Welch KM, Zivin JA. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355:549–559. - PubMed
-
- Goldstein LB, Amarenco P, Zivin J, Messig M, Altafullah I, Callahan A, Hennerici M, MacLeod MJ, Sillesen H, Zweifler R, Michael K, Welch A. Statin treatment and stroke outcome in the stroke prevention by aggressive reduction in cholesterol levels (sparcl) trial. Stroke. 2009;40:3526–3531. - PubMed
-
- Greisenegger S, Mullner M, Tentschert S, Lang W, Lalouschek W. Effect of pretreatment with statins on the severity of acute ischemic cerebrovascular events. J Neurol Sci. 2004;221:5–10. - PubMed
-
- Marti-Fabregas J, Gomis M, Arboix A, Aleu A, Pagonabarraga J, Belvis R, Cocho D, Roquer J, Rodriguez A, Garcia MD, Molina-Porcel L, Diaz-Manera J, Marti-Vilalta JL. Favorable outcome of ischemic stroke in patients pretreated with statins. Stroke. 2004;35:1117–1121. - PubMed
-
- Reeves MJ, Gargano JW, Luo Z, Mullard AJ, Jacobs BS, Majid A. Effect of pretreatment with statins on ischemic stroke outcomes. Stroke. 2008;39:1779–1785. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
