

'Sink or swim': an evaluation of the clinical characteristics of individuals with high bone mass
- PMID: 21455762
- PMCID: PMC3261396
- DOI: 10.1007/s00198-011-1603-4
'Sink or swim': an evaluation of the clinical characteristics of individuals with high bone mass
Abstract
Summary: High bone mineral density on routine dual energy X-ray absorptiometry (DXA) may indicate an underlying skeletal dysplasia. Two hundred fifty-eight individuals with unexplained high bone mass (HBM), 236 relatives (41% with HBM) and 58 spouses were studied. Cases could not float, had mandible enlargement, extra bone, broad frames, larger shoe sizes and increased body mass index (BMI). HBM cases may harbour an underlying genetic disorder.
Introduction: High bone mineral density is a sporadic incidental finding on routine DXA scanning of apparently asymptomatic individuals. Such individuals may have an underlying skeletal dysplasia, as seen in LRP5 mutations. We aimed to characterize unexplained HBM and determine the potential for an underlying skeletal dysplasia.
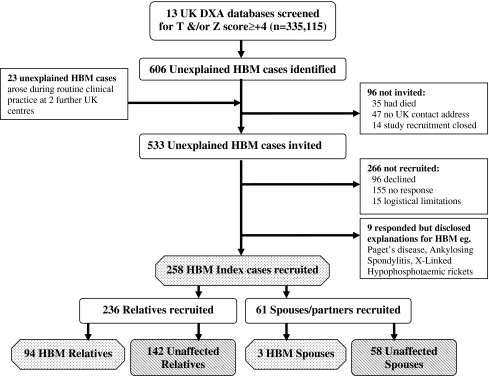
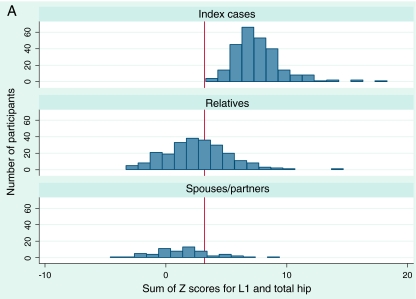
Methods: Two hundred fifty-eight individuals with unexplained HBM (defined as L1 Z-score ≥ +3.2 plus total hip Z-score ≥ +1.2, or total hip Z-score ≥ +3.2) were recruited from 15 UK centres, by screening 335,115 DXA scans. Unexplained HBM affected 0.181% of DXA scans. Next 236 relatives were recruited of whom 94 (41%) had HBM (defined as L1 Z-score + total hip Z-score ≥ +3.2). Fifty-eight spouses were also recruited together with the unaffected relatives as controls. Phenotypes of cases and controls, obtained from clinical assessment, were compared using random-effects linear and logistic regression models, clustered by family, adjusted for confounders, including age and sex.
Results: Individuals with unexplained HBM had an excess of sinking when swimming (7.11 [3.65, 13.84], p < 0.001; adjusted odds ratio with 95% confidence interval shown), mandible enlargement (4.16 [2.34, 7.39], p < 0.001), extra bone at tendon/ligament insertions (2.07 [1.13, 3.78], p = 0.018) and broad frame (3.55 [2.12, 5.95], p < 0.001). HBM cases also had a larger shoe size (mean difference 0.4 [0.1, 0.7] UK sizes, p = 0.009) and increased BMI (mean difference 2.2 [1.3, 3.1] kg/m(2), p < 0.001).
Conclusion: Individuals with unexplained HBM have an excess of clinical characteristics associated with skeletal dysplasia and their relatives are commonly affected, suggesting many may harbour an underlying genetic disorder affecting bone mass.
Figures
References
-
- Cherian RA, Haddaway MJ, Davie MW, McCall IW, Cassar-Pullicino VN. Effect of Paget’s disease of bone on areal lumbar spine bone mineral density measured by DXA, and density of cortical and trabecular bone measured by quantitative CT. Br J Radiol. 2000;73:720–726. - PubMed
-
- Gregson CL, Tobias JH. Interpretation of high bone mineral density measurements. Osteoporos Rev. 2007;15:2–6.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
