

Prophylactic 5-Fr pancreatic duct stents are superior to 3-Fr stents: a randomized controlled trial
- PMID: 21455872
- PMCID: PMC3514442
- DOI: 10.1055/s-0030-1256305
Prophylactic 5-Fr pancreatic duct stents are superior to 3-Fr stents: a randomized controlled trial
Abstract
Background: Temporary prophylactic pancreatic duct stenting effectively reduces post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis (PEP) in high-risk patients, but the optimal stent remains unclear. We compared rate of spontaneous passage, and technical difficulty of placement for 3-Fr and 5-Fr stents.
Methods: A randomized controlled trial at a single academic medical center. Patients deemed high risk for PEP randomly received 5-Fr or 3-Fr pancreatic duct stents. Primary outcome was spontaneous stent passage by 2 weeks. Secondary outcomes were ease and time for stent placement, and number of guide wires required for the entire procedure.
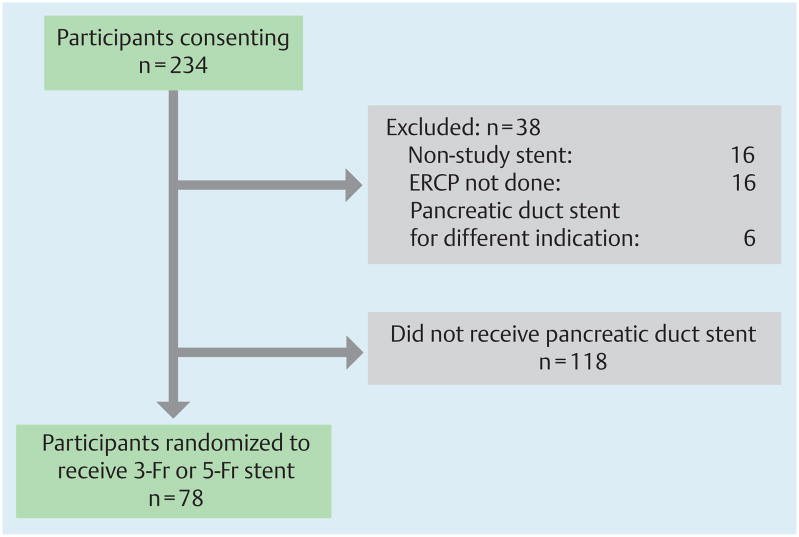
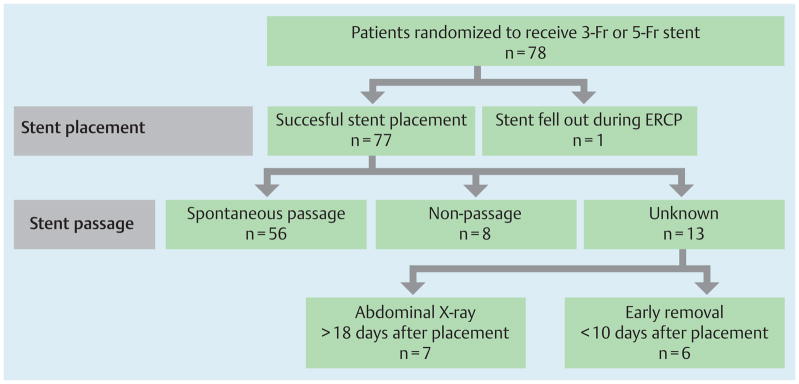
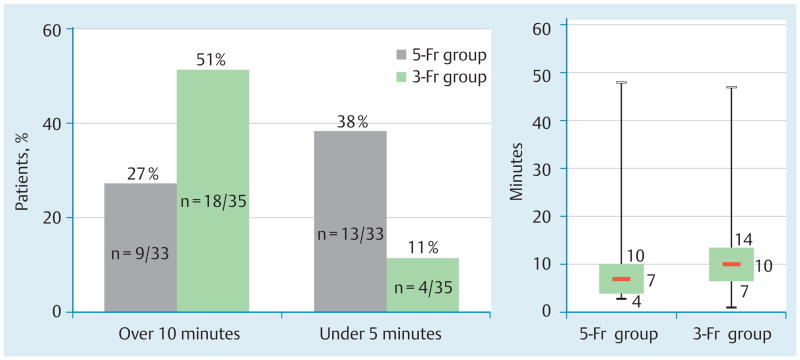
Results: Patients (69 female [89 %]; mean age 44.9 years, standard deviation [SD] 16.8) were randomly assigned to receive 5-Fr (n = 38) and 3-Fr (n = 40) stents. Indications for stenting were similar. Seven patients in the 3-Fr group actually received a 5-Fr stent, and two in the 5-Fr group had a 3-Fr stent. Spontaneous passage or non-passage was confirmed in 64 (83 %). No statistically significant difference in spontaneous passage rates was seen (5-Fr group, 68.4 %; 3-Fr group 75.0 %; P = 0.617). Non-passage rates were 10.5 % (5-Fr group) and 10.0 % (3-Fr group) ( P = 1.00). The study was stopped after a futility analysis for the primary end point. Placement of 5-Fr stents was rated easier, at a mean score of 1.8 (5-Fr) vs. 3.4 (3-Fr), P < 0.001, with a trend towards being faster, 9.2 vs. 11.1 minutes ( P = 0.355). Fewer guide wires were required for 5-Fr stent placement, 1.5 vs. 1.9 ( P = 0.002). PEP rates did not differ ( P = 0.519).
Conclusion: Placement of 5-Fr compared to 3-Fr pancreatic duct stents for PEP prophylaxis is easier, faster, and requires fewer wires. No statistically significant difference in spontaneous passage was found between the two sizes.
© Georg Thieme Verlag KG Stuttgart · New York.
Conflict of interest statement
Figures
Comment in
-
Pancreatic endoscopic retrograde cholangiopancreatography (ERCP).Endoscopy. 2012 Apr;44(4):389-93. doi: 10.1055/s-0031-1291872. Epub 2012 Mar 21. Endoscopy. 2012. PMID: 22438149 No abstract available.
References
-
- Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393. - PubMed
-
- Fazel A, Quadri A, Catalano MF, et al. Does a pancreatic duct stent prevent post-ERCP pancreatitis? A prospective randomized study. Gastrointest Endosc. 2003;57:291–294. - PubMed
-
- Singh P, Das A, Isenberg G, et al. Does prophylactic pancreatic stent placement reduce the risk of post-ERCP acute pancreatitis? A meta-analysis of controlled trials. Gastrointest Endosc. 2004;60:544–550. - PubMed
-
- Aizawa T, Ueno N. Stent placement in the pancreatic duct prevents pancreatitis after endoscopic sphincter dilation for removal of bile duct stones. Gastrointest Endosc. 2001;54:209–213. - PubMed
-
- Smithline A, Silverman W, Rogers D, et al. Effect of prophylactic main pancreatic duct stenting on the incidence of biliary endoscopic sphincterotomy-induced pancreatitis in high-risk patients. Gastrointest Endosc. 1993;39:652–657. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
