

Indoor particulate matter increases asthma morbidity in children with non-atopic and atopic asthma
- PMID: 21457879
- PMCID: PMC3118306
- DOI: 10.1016/j.anai.2011.01.015
Indoor particulate matter increases asthma morbidity in children with non-atopic and atopic asthma
Abstract
Background: Compared with atopic asthma, fewer environmental modifications are recommended for non-atopic asthma in children.
Objective: To better understand the role of indoor pollutants in provoking non-atopic asthma, we investigated the effect of in-home particulate matter on asthma symptoms among non-atopic and atopic children living in inner-city Baltimore.
Methods: A cohort of 150 children ages 2 to 6 years with asthma underwent home environmental monitoring for 3-day intervals at baseline, 3, and 6 months. Children were classified as non-atopic if they were skin test negative to a panel of 14 aeroallergens. Caregivers completed questionnaires assessing symptoms and rescue medication use. Longitudinal data analysis included regression models with generalized estimating equations.
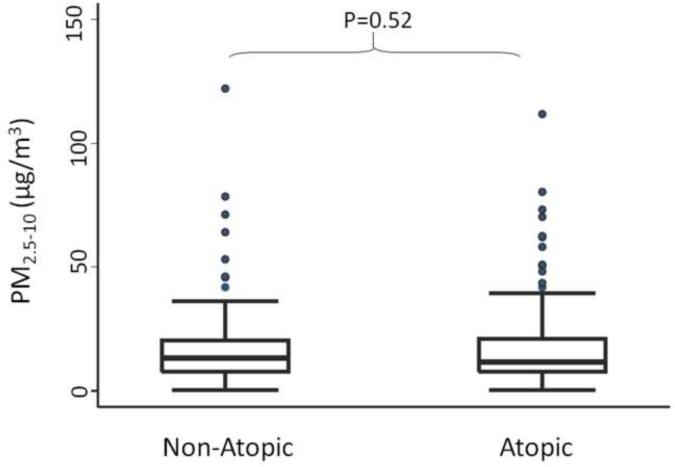
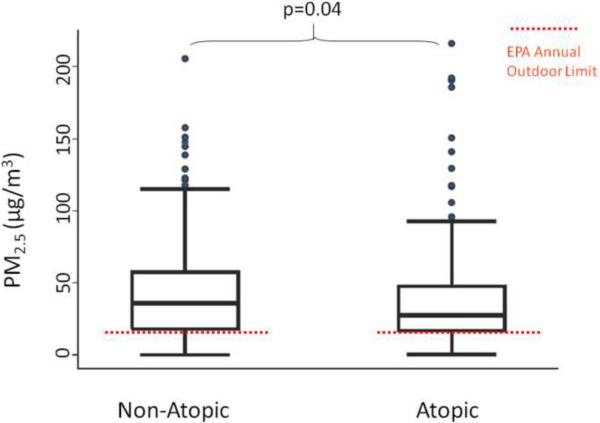
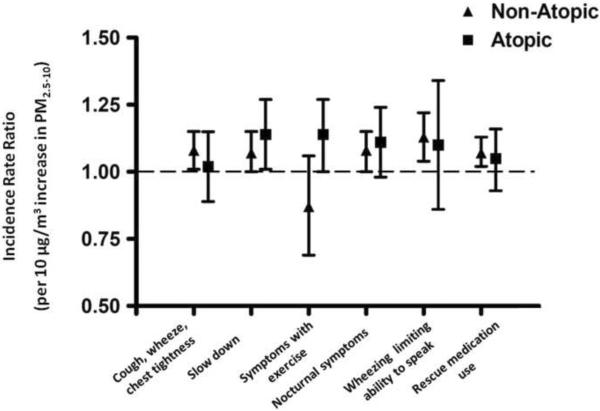
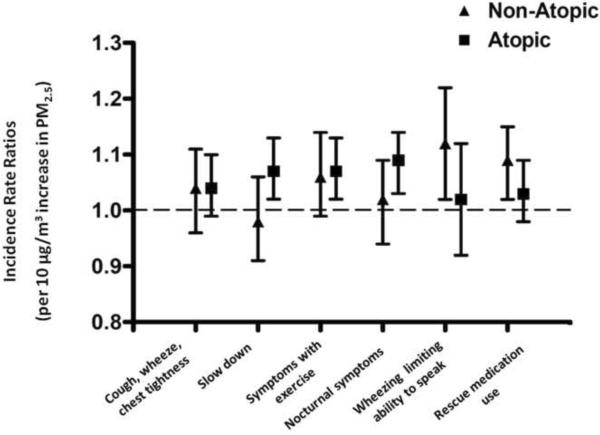
Results: Children were primarily African American from lower socioeconomic backgrounds and spent most of their time in the home. Thirty-one percent were non-atopic, and 69% were atopic. Among non-atopic and atopic children, increased in-home fine (PM2.5) and coarse (PM2.5-10) particle concentrations were associated with significant increases in asthma symptoms and rescue medication use ranging from 7% (95% confidence interval [CI], 0-15) to 14% (95% CI, 1-27) per 10 μg/m(3) increase in particle concentration after adjustment for confounders.
Conclusions: In-home particles similarly cause increased symptoms of asthma in non-atopic and atopic children. Environmental control strategies that reduce particle concentrations may prove to be an effective means of improving asthma outcomes, especially for non-atopic asthma, for which there are few environmental control practice recommendations.
Copyright © 2011. Published by Elsevier Inc.
Figures
References
-
- Beasley R, Pekkanen J, Pearce N. Has the role of atopy in the development of asthma been over-emphasized? Pediatr Pulmonol. 2001;(Suppl 23):149–150. - PubMed
-
- Ostergaard PA. Non-IgE-mediated asthma in children. Acta Paediatr Scand. 1985;74(5):713–719. - PubMed
-
- Longo G, Panontin E, Ventura G. Non-atopic persistent asthma in children. Thorax. 2009;64(5):459. - PubMed
