

Metabolic syndrome and renal injury
- PMID: 21461396
- PMCID: PMC3065010
- DOI: 10.4061/2011/567389
Metabolic syndrome and renal injury
Abstract
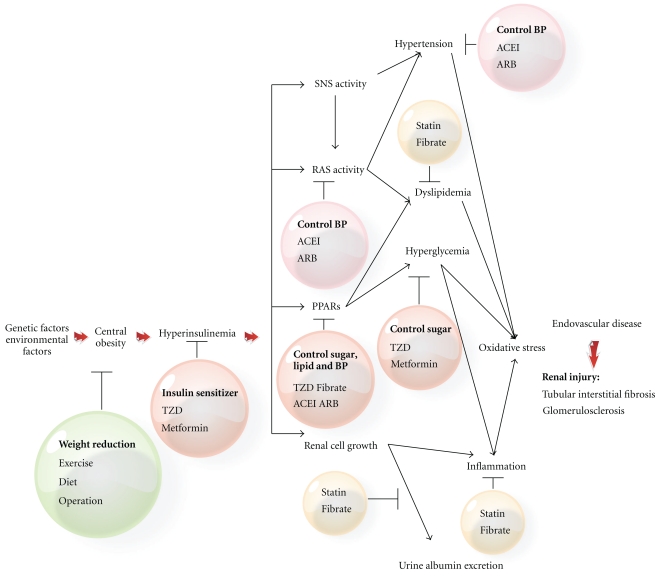
Both metabolic syndrome (MetS) and chronic kidney disease (CKD) are major global health issues. Current clinical markers used to reflect renal injury include albuminuria and estimated glomerular filtration rate (eGFR). Given the same eGFR level, urine albumin might be a better risk marker to predict progression of CKD and future development of cardiovascular diseases (CVDs). Serum Cystatin C is emerging as a new biomarker for early detection of renal injury associated with MetS and cardiovascular risk. In addition to each component, MetS per se influences the incidence and prognosis of renal injury and the odds ratios increased with the increase in the number of metabolic abnormalities. Hyperinsulinemia, activation of rennin-angiotensin-aldosterone system, increase of oxidative stress, and inflammatory cytokines are proposed to be the plausible biological link between MetS and CKD. Weight control, stick control of blood pressure, glucose, and lipids disorders may lead to lessening renal injury and even the subsequent CVD.
Figures
Similar articles
-
Association of Metabolic Syndrome with Chronic Kidney Disease in Elderly Japanese Women: Comparison by Estimation of Glomerular Filtration Rate from Creatinine, Cystatin C, and Both.Metab Syndr Relat Disord. 2016 Feb;14(1):40-5. doi: 10.1089/met.2015.0085. Epub 2015 Nov 4. Metab Syndr Relat Disord. 2016. PMID: 26535975
-
[Associations of metabolic score for insulin resistance with chronic kidney disease and albuminuria in the Chinese population].Zhonghua Nei Ke Za Zhi. 2023 Mar 1;62(3):281-289. doi: 10.3760/cma.j.cn112138-20220420-00288. Zhonghua Nei Ke Za Zhi. 2023. PMID: 36822854 Chinese.
-
Metabolic syndrome and chronic kidney disease: Current status and future directions.World J Nephrol. 2014 Nov 6;3(4):210-9. doi: 10.5527/wjn.v3.i4.210. World J Nephrol. 2014. PMID: 25374814 Free PMC article. Review.
-
The kidney and cardiovascular outcome trials.J Diabetes. 2018 Feb;10(2):88-89. doi: 10.1111/1753-0407.12616. J Diabetes. 2018. PMID: 29031006
-
Subclinical Kidney Damage in Hypertensive Patients: A Renal Window Opened on the Cardiovascular System. Focus on Microalbuminuria.Adv Exp Med Biol. 2017;956:279-306. doi: 10.1007/5584_2016_85. Adv Exp Med Biol. 2017. PMID: 27873229 Review.
Cited by
-
A triglyceride-rich lipoprotein environment exacerbates renal injury in the accelerated nephrotoxic nephritis model.Clin Exp Immunol. 2018 Jun;192(3):337-347. doi: 10.1111/cei.13111. Epub 2018 Mar 9. Clin Exp Immunol. 2018. PMID: 29405270 Free PMC article.
-
Peripheral arterial stiffness is independently associated with a rapid decline in estimated glomerular filtration rate in patients with type 2 diabetes.Biomed Res Int. 2013;2013:309294. doi: 10.1155/2013/309294. Epub 2013 Dec 29. Biomed Res Int. 2013. PMID: 24471138 Free PMC article.
-
Metabolic syndrome leading to chronic kidney disease: An emerging threat.Indian J Endocrinol Metab. 2012 Mar;16(2):151-3. doi: 10.4103/2230-8210.93728. Indian J Endocrinol Metab. 2012. PMID: 22470847 Free PMC article. No abstract available.
-
Activation of angiotensin-converting enzyme 2 ameliorates metabolic syndrome-induced renal damage in rats by renal TLR4 and nuclear transcription factor κB downregulation.Front Med (Lausanne). 2022 Aug 12;9:904756. doi: 10.3389/fmed.2022.904756. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36035416 Free PMC article.
References
-
- Pei D, Kuo SW, Wu DA, et al. The relationships between insulin resistance and components of metabolic syndrome in Taiwanese Asians. International Journal of Clinical Practice. 2005;59(12):1408–1416. - PubMed
-
- Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement—executive summary. Critical Pathways in Cardiology. 2005;4(4):198–203. - PubMed
-
- Sheu WHH, Chuang SY, Lee WJ, Tsai ST, Chou P, Chen CH. Predictors of incident diabetes, metabolic syndrome in middle-aged adults: a 10-year follow-up study from Kinmen, Taiwan. Diabetes Research and Clinical Practice. 2006;74(2):162–168. - PubMed
-
- Iglesias P, Díez JJ. Adipose tissue in renal disease: clinical significance and prognostic implications. Nephrology Dialysis Transplantation. 2010;25(7):2066–2077. - PubMed
-
- Rosito GA, Massaro JM, Hoffmann U, et al. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample the framingham heart study. Circulation. 2008;117(5):605–613. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
