

Pharmacotherapy of vestibular and ocular motor disorders, including nystagmus
- PMID: 21461686
- PMCID: PMC3132281
- DOI: 10.1007/s00415-011-5999-8
Pharmacotherapy of vestibular and ocular motor disorders, including nystagmus
Abstract
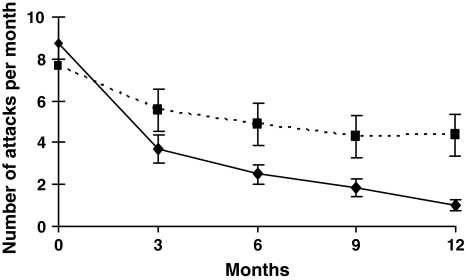
We review current pharmacological treatments for peripheral and central vestibular disorders, and ocular motor disorders that impair vision, especially pathological nystagmus. The prerequisites for successful pharmacotherapy of vertigo, dizziness, and abnormal eye movements are the "4 D's": correct diagnosis, correct drug, appropriate dosage, and sufficient duration. There are seven groups of drugs (the "7 A's") that can be used: antiemetics; anti-inflammatory, anti-Ménière's, and anti-migrainous medications; anti-depressants, anti-convulsants, and aminopyridines. A recovery from acute vestibular neuritis can be promoted by treatment with oral corticosteroids. Betahistine may reduce the frequency of attacks of Ménière's disease. The aminopyridines constitute a novel treatment approach for downbeat and upbeat nystagmus, as well as episodic ataxia type 2 (EA 2); these drugs may restore normal "pacemaker" activity to the Purkinje cells that govern vestibular and cerebellar nuclei. A limited number of trials indicate that baclofen improves periodic alternating nystagmus, and that gabapentin and memantine improve acquired pendular and infantile (congenital) nystagmus. Preliminary reports suggest suppression of square-wave saccadic intrusions by memantine, and ocular flutter by beta-blockers. Thus, although progress has been made in the treatment of vestibular neuritis, some forms of pathological nystagmus, and EA 2, controlled, masked trials are still needed to evaluate treatments for many vestibular and ocular motor disorders, including betahistine for Ménière's disease, oxcarbazepine for vestibular paroxysmia, or metoprolol for vestibular migraine.
Figures



References
-
- Neuhauser HK. Epidemiology of vertigo. Curr Opin Neurol. 2007;20:40–46. - PubMed
-
- Brandt T, Dieterich M, Strupp M. Vertigo and dizziness—common complaints. London: Springer; 2005.
-
- Strupp M, Cnyrim C, Brandt T. Vertigo and dizziness: Treatment of benign paroxysmal positioning vertigo, vestibular neuritis and Menère’s disease. In: Candelise L, editor. Evidence-based Neurology—management of neurological disorders. Oxford: Blackwell Publishing; 2007. pp. 59–69.
-
- Leigh RJ, Zee D. The neurology of eye movements. 4. Oxford: Oxford University Press; 2006.
-
- Straube A. Therapeutic considerations for eye movement disorders. Dev Ophthalmol. 2007;40:175–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
