

Vascular time-activity variation in patients undergoing ¹²³I-MIBG myocardial scintigraphy: implications for quantification of cardiac and mediastinal uptake
- PMID: 21461736
- PMCID: PMC3094534
- DOI: 10.1007/s00259-011-1783-3
Vascular time-activity variation in patients undergoing ¹²³I-MIBG myocardial scintigraphy: implications for quantification of cardiac and mediastinal uptake
Abstract
Purpose: For the quantification of cardiac (123)I-metaiodobenzylguanidine (MIBG) uptake, the mediastinum is commonly used as a reference region reflecting nonspecific background activity. However, variations in the quantity of vascular structures in the mediastinum and the rate of renal clearance of (123)I-MIBG from the blood pool may contribute to increased interindividual variation in uptake. This study examined the relationship between changes in heart (H) and mediastinal (M) counts and the change in vascular (123)I-MIBG activity, including the effect of renal function.
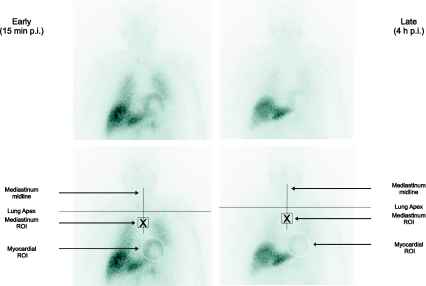
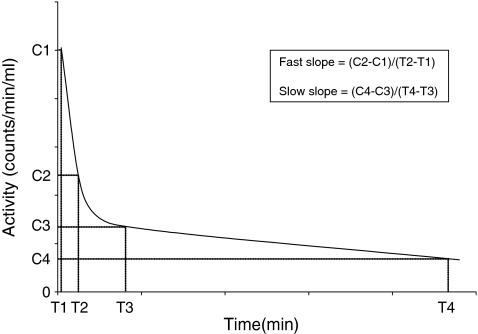
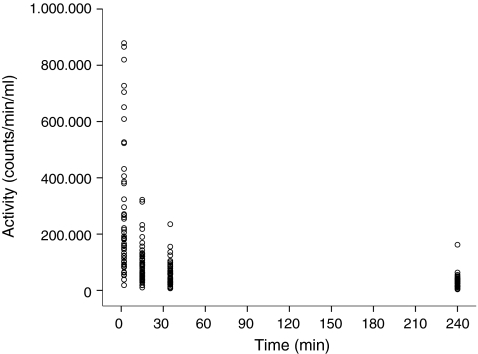
Methods: Fifty-one subjects with ischemic heart disease underwent early (15 min) and late (4 h) anterior planar images of the chest following injection of (123)I-MIBG. Vascular (123)I-MIBG activity was determined from venous blood samples obtained at 2 min, 15 min, 35 min, and 4 h post-injection. From the vascular clearance curve of each subject, the mean blood counts/min per ml at the time of each acquisition and the slope of the clearance curve were determined. Renal function was expressed as the estimated creatinine clearance (e-CC) and the estimated glomerular filtration rate (e-GFR). Relations between H and M region of interest (ROI) counts/pixel, vascular activity, and renal function were then examined using linear regression.
Results: Changes in ROI activity ratios between early and late planar images could not be explained by blood activity, the slope of the vascular clearance curves, or estimates of renal function. At most 3% of the variation in image counts could be explained by changes in vascular activity (p = 0.104). The e-CC and e-GFR could at best explain approximately 1.5% of the variation in the slopes of the vascular clearance curve (p = 0.194).
Conclusion: The change in measured H and M counts between early and late planar (123)I-MIBG images is unrelated to intravascular levels of the radiopharmaceutical. This suggests that changes in M counts are primarily due to decrease in soft tissue activity and scatter from the adjacent lungs.
Figures
Similar articles
-
Impact of mediastinal, liver and lung (123)I-metaiodobenzylguanidine ( (123)I-MIBG) washout on calculated (123)I-MIBG myocardial washout.Eur J Nucl Med Mol Imaging. 2009 Aug;36(8):1322-8. doi: 10.1007/s00259-009-1093-1. Epub 2009 Mar 4. Eur J Nucl Med Mol Imaging. 2009. PMID: 19259662 Free PMC article.
-
¹²³I-MIBG heart-to-mediastinum ratio is influenced by high-energy photon penetration of collimator septa from liver and lung activity.Nucl Med Commun. 2015 Mar;36(3):279-85. doi: 10.1097/MNM.0000000000000238. Nucl Med Commun. 2015. PMID: 25415845 Clinical Trial.
-
Influence of myocardial region of interest definition on quantitative analysis of planar 123I-mIBG images.Eur J Nucl Med Mol Imaging. 2013 Apr;40(4):558-64. doi: 10.1007/s00259-012-2336-0. Epub 2013 Jan 29. Eur J Nucl Med Mol Imaging. 2013. PMID: 23359065
-
[Assessment of most appropriate background subtraction method for quantification of 123I-metaiodobenzylguanidine (MIBG) myocardial uptake by comparing with plasma ANP and BNP].Kaku Igaku. 2000 May;37(3):217-25. Kaku Igaku. 2000. PMID: 10860352 Japanese.
-
Quantification and Determination of Normal 123I-Meta Iodobenzylguanidine Heart-to-Mediastinum Ratio (HMR) from Cardiac SPECT/CT and Correlation with Planar HMR.J Nucl Med. 2018 Apr;59(4):652-658. doi: 10.2967/jnumed.117.197152. Epub 2017 Sep 15. J Nucl Med. 2018. PMID: 28916622 Clinical Trial.
Cited by
-
Renal Function in Relation to Cardiac (123)I-MIBG Scintigraphy in Patients with Chronic Heart Failure.Int J Mol Imaging. 2012;2012:434790. doi: 10.1155/2012/434790. Epub 2012 May 14. Int J Mol Imaging. 2012. PMID: 22666580 Free PMC article.
-
Predictive impacts of chronic kidney disease and cardiac sympathetic nervous activity on lethal arrhythmic events in chronic heart failure.Ann Noninvasive Electrocardiol. 2022 Jan;27(1):e12900. doi: 10.1111/anec.12900. Epub 2021 Oct 22. Ann Noninvasive Electrocardiol. 2022. PMID: 34676627 Free PMC article.
-
Assessment of global cardiac I-123 MIBG uptake and washout using volumetric quantification of SPECT acquisitions.J Nucl Cardiol. 2012 Aug;19(4):752-62. doi: 10.1007/s12350-012-9539-4. Epub 2012 Jun 6. J Nucl Cardiol. 2012. PMID: 22669736 Free PMC article.
-
Renal sympathetic nerve activity after catheter-based renal denervation.EJNMMI Res. 2018 Jan 26;8(1):8. doi: 10.1186/s13550-018-0360-1. EJNMMI Res. 2018. PMID: 29374335 Free PMC article.
References
-
- Agostini D, Verberne HJ, Burchert W, Knuuti J, Povinec P, Sambuceti G, et al. I-123-mIBG myocardial imaging for assessment of risk for a major cardiac event in heart failure patients: insights from a retrospective European multicenter study. Eur J Nucl Med Mol Imaging. 2008;35:535–546. doi: 10.1007/s00259-007-0639-3. - DOI - PubMed
-
- Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol. 2010;55:2212–2221. doi: 10.1016/j.jacc.2010.01.014. - DOI - PubMed
-
- Kline RC, Swanson DP, Wieland DM, Thrall JH, Gross MD, Pitt B, et al. Myocardial imaging in man with I-123 meta-iodobenzylguanidine. J Nucl Med. 1981;22:129–132. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
