

Anomalous origin of the left coronary artery from the pulmonary artery in adults: a comprehensive review of 151 adult cases and a new diagnosis in a 53-year-old woman
- PMID: 21462214
- PMCID: PMC6652342
- DOI: 10.1002/clc.20848
Anomalous origin of the left coronary artery from the pulmonary artery in adults: a comprehensive review of 151 adult cases and a new diagnosis in a 53-year-old woman
Abstract
Background: Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital coronary abnormality associated with early infant mortality and adult sudden death. As it predominantly presents in the first year of life, diagnosis in living adults is extremely rare. Current management is based on limited case series or extrapolated from pediatric cases. Modern advances in noninvasive cardiac imaging have substantially increased the number of diagnoses, uncovering a large adult population that has not been reviewed.
Hypothesis: The availability of newer diagnostic modalities correlates with an increasing incidence in an older cohort, and true association between sudden death and ALCAPA may be lower, especially among older patients.
Methods: A comprehensive literature search was performed for all case reports of ALCAPA on MEDLINE and PubMed using the keywords ALCAPA, Bland-White-Garland, and coronary anomaly; and augmented by references from published case reports from 1908 to 2008. All adult cases, defined by age 18 years and older, were reviewed for this article.
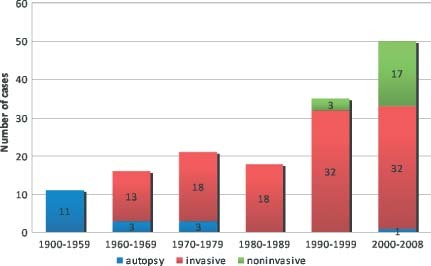
Results: One hundred fifty-one adult cases of ALCAPA are described, in addition to the case of an asymptomatic 53-year-old woman. The average reported age was 41 years old with the oldest being 83. Sixty-six percent of the patients presented with symptoms of angina, dyspnea, palpitations, or fatigue; 17% presented with ventricular arrhythmia, syncope, or sudden death; and 14% were asymptomatic. Twelve percent were diagnosed at autopsy. The majority had some form of surgical correction during their clinical course.
Conclusions: ALCAPA is a rare and life-threatening condition in adults. The availability of newer, less invasive diagnostic modalities has resulted in more frequent identification of this condition in an older cohort.
© 2011 Wiley Periodicals, Inc.
Figures
References
-
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28–40. - PubMed
-
- Frescura C, Basso C, Thiene G, et al. Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart disease. Hum Pathol. 1998;29: 689–695. - PubMed
-
- Konstantinowitsch W. Ein seltener Fall von Herzmissbildung. Prager med Wchnschr. 1906;31:657–660.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
