

Event-free survival following CRT with surgically implanted LV leads versus standard transvenous approach
- PMID: 21463344
- PMCID: PMC3079428
- DOI: 10.1111/j.1540-8159.2010.03014.x
Event-free survival following CRT with surgically implanted LV leads versus standard transvenous approach
Abstract
Background: While surgical epicardial lead placement is performed in a subset of cardiac resynchronization therapy patients, data comparing survival following surgical versus transvenous lead placement are limited. We hypothesized that surgical procedures would be associated with increased mortality risk.
Methods: Long-term event-free survival was assessed for 480 consecutive patients undergoing surgical (48) or percutaneous (432) left ventricle (LV) lead placement at our institution from January 2000 to September 2008.
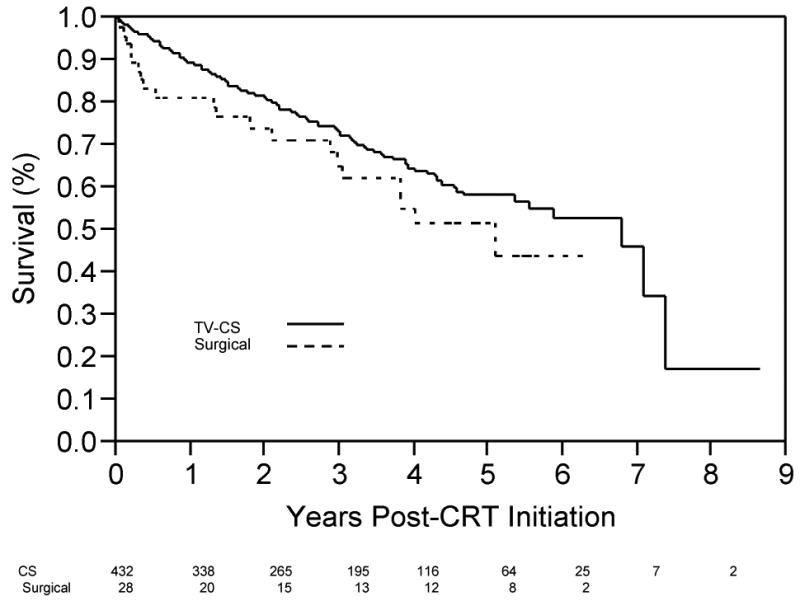
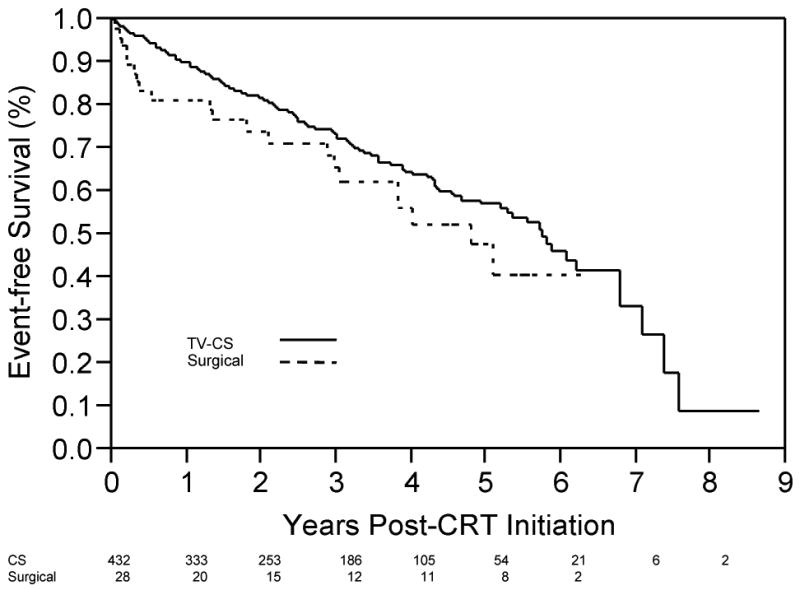
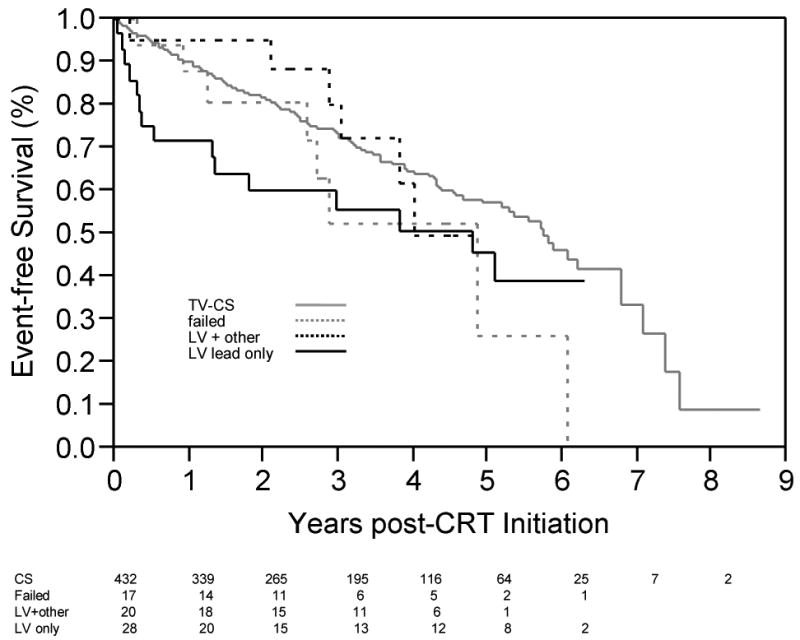
Results: Baseline clinical and demographic characteristics were similar between groups. While there was no statistically significant difference in overall event-free survival (P = 0.13), when analysis was restricted to surgical patients with isolated surgical lead placement (n = 28), event-free survival was significantly lower in surgical patients (P = 0.015). There appeared to be an early risk (first approximately 3 months postimplantation) with surgical lead placement, primarily in LV lead-only patients. Event rates were significantly higher in LV lead-only surgical patients than in transvenous patients in the first 3 months (P = 0.006). In proportional hazards analysis comparing isolated surgical LV lead placement to transvenous lead placement, adjusted hazard ratios were 1.8 ([1.1,2.7] P = 0.02) and 1.3 ([1.0,1.7] P = 0.07) for the first 3 months and for the full duration of follow-up, respectively.
Conclusions: Isolated surgical LV lead placement appears to carry a small but significant upfront mortality cost, with risk extending beyond the immediate postoperative period. Long-term survival is similar, suggesting those surviving beyond this period of early risk derive the same benefit as coronary sinus lead recipients. Further work is needed to identify risk factors associated with early mortality following surgical lead placement.
©2011, The Authors. Journal compilation ©2011 Wiley Periodicals, Inc.
Figures
References
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NAM, III, Freedman RA, Gettes LS, Gillinov AM, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;51:e1–62. - PubMed
-
- Auricchio A, Stellbrink C, Sack S, Block M, Vogt J, Bakker P, Huth C, et al. Long-term clinical effect of hemodynamically optimized cardiac resynchronization therapy in patients with heart failure and ventricular conduction delay. Journal of the American College of Cardiology. 2002;39:2026–2033. - PubMed
-
- Higgins SL, Hummel JD, Niazi IK, Giudici MC, Worley SJ, Saxon LA, Boehmer JP, et al. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. Journal of the American College of Cardiology. 2003;42:1454–1459. - PubMed
-
- Higgins SL, Yong P, Scheck D, McDaniel M, Bollinger F, Vadecha M, Desai S, et al. Biventricular pacing diminishes the need for implantable cardioverter defibrillator therapy. Journal of the American College of Cardiology. 2000;36:824–827. - PubMed
-
- McAlister FA, Ezekowitz JA, Wiebe N, Rowe B, Spooner C, Crumley E, Hartling L, et al. Systematic Review: Cardiac Resynchronization in Patients with Symptomatic Heart Failure. Annals of Internal Medicine. 2004;141 381-W-375. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
