

Surgeon-performed ultrasound is superior to 99Tc-sestamibi scanning to localize parathyroid adenomas in patients with primary hyperparathyroidism: results in 516 patients over 10 years
- PMID: 21463783
- PMCID: PMC5706459
- DOI: 10.1016/j.jamcollsurg.2010.12.038
Surgeon-performed ultrasound is superior to 99Tc-sestamibi scanning to localize parathyroid adenomas in patients with primary hyperparathyroidism: results in 516 patients over 10 years
Abstract
Background: Surgeon-performed cervical ultrasound (SUS) and 99Tc-sestamibi scanning (MIBI) are both useful in patients with primary hyperparathyroidism (PHPT). We sought to determine the relative contributions of SUS and MIBI to accurately predict adenoma location.
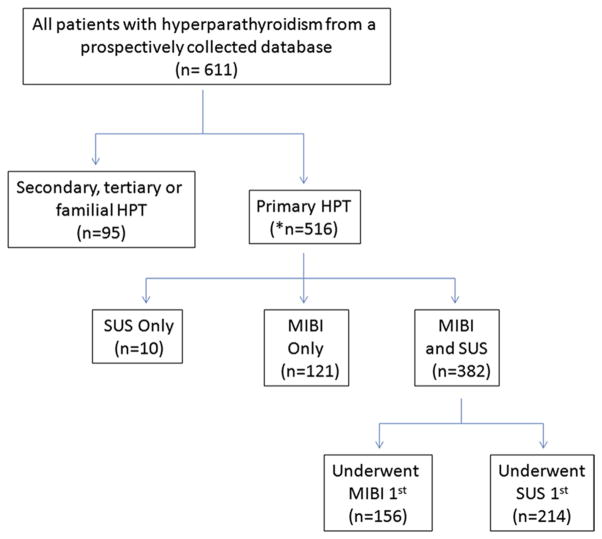
Study design: We performed a database review of 516 patients undergoing surgery for PHPT between 2001 and 2010. SUS was performed by 1 of 3 endocrine surgeons. MIBI used 2-hour delayed anterior planar and single-photon emission computerized tomography images. Directed parathyroidectomy was performed with extent of surgery governed by intraoperative parathyroid hormone decline of 50%.
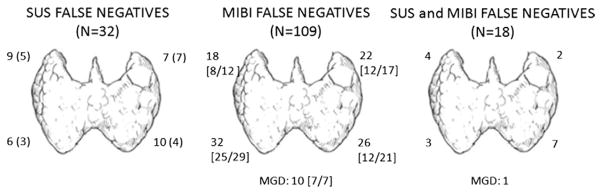
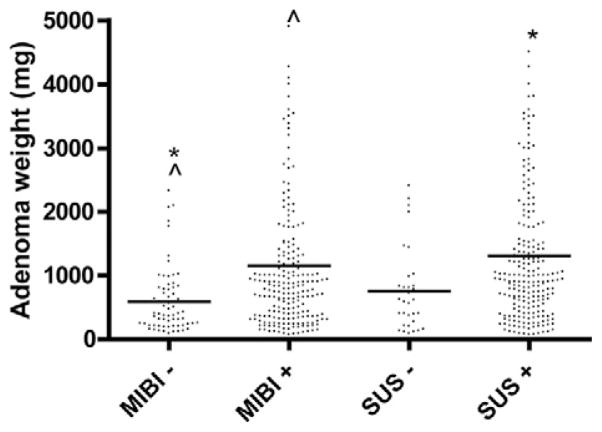
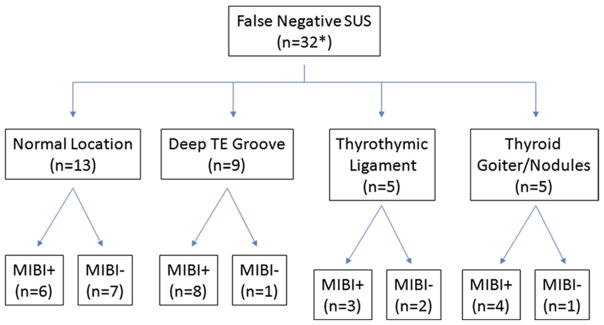
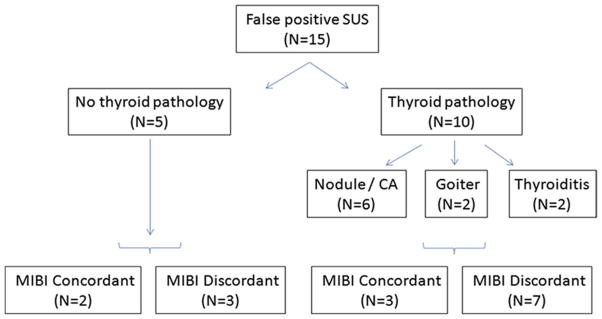
Results: SUS accurately localized adenomas in 87% of patients (342/392), and MIBI correctly identified their locations in 76%, 383/503 (p < 0.001). In patients who underwent SUS first, MIBI provided no additional information in 92% (144/156). In patients who underwent MIBI first, 82% of the time (176/214) SUS was unnecessary (p = 0.015). In 32 patients SUS was falsely negative. The reason for these included gland location in either the deep tracheoesophageal groove (n = 9) or the thyrothymic ligament below the clavicle (n = 5), concurrent thyroid goiter (n = 4), or thyroid cancer (n = 1). In 13 cases, the adenoma was located in a normal ultrasound-accessible location but was missed by the preoperative exam. In the 32 ultrasound false-negative cases, MIBI scans were positive in 21 (66%). Of the 516 patients, 7.6% had multigland disease. Persistent disease occurred in 4 patients (1%) and recurrent disease occurred in 6 (1.2%).
Conclusions: When performed by experienced surgeons, SUS is more accurate than MIBI for predicting the location of abnormal parathyroids in PHPT patients. For patients facing first-time surgery for PHPT, we now reserve MIBI for patients with unclear or negative SUS.
Copyright © 2011 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Coakley AJ, Kettle AG, Wells CP, et al. 99Tcm sestamibi—a new agent for parathyroid imaging. Nucl Med Commun. 1989;10:791–794. - PubMed
-
- Gotthardt M, Lohmann B, Behr TM, et al. Clinical value of parathyroid scintigraphy with technetium-99m methoxyisobutylisonitrile: discrepancies in clinical data and a systematic meta-analysis of the literature. World J Surg. 2004;28:100–107. - PubMed
-
- Siperstein A, Berber E, Mackey R, et al. Prospective evaluation of sestamibi scan, ultrasonography, and rapid PTH to predict the success of limited exploration for sporadic primary hyperparathyroidism. Surgery. 2004;136:872–880. - PubMed
-
- Solorzano CC, Carneiro-Pla DM, Irvin GL., 3rd Surgeon-performed ultrasonography as the initial and only localizing study in sporadic primary hyperparathyroidism. J Am Coll Surg. 2006;202:18–24. - PubMed
-
- Miller BS, Gauger PG, Broome JT, et al. An international perspective on ultrasound training and use for thyroid and parathyroid disease. World J Surg. 2010;34:1157–1163. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
