

Disorder-specific impact of coordinated anxiety learning and management treatment for anxiety disorders in primary care
- PMID: 21464362
- PMCID: PMC3074172
- DOI: 10.1001/archgenpsychiatry.2011.25
Disorder-specific impact of coordinated anxiety learning and management treatment for anxiety disorders in primary care
Abstract
Context: Anxiety disorders commonly present in primary care, where evidence-based mental health treatments often are unavailable or suboptimally delivered.
Objective: To compare evidence-based treatment for anxiety disorders with usual care (UC) in primary care for principal and comorbid generalized anxiety disorder (GAD), panic disorder (PD), social anxiety disorder (SAD), and posttraumatic stress disorder (PTSD).
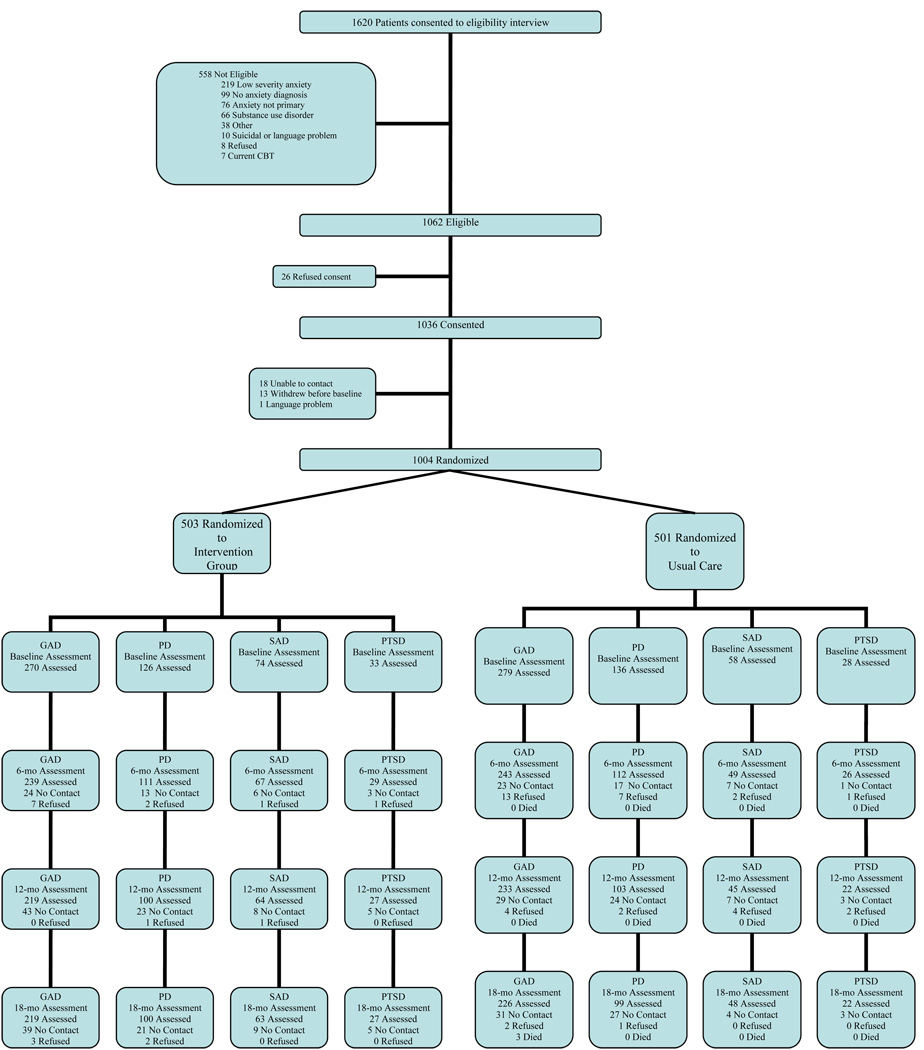
Design: A randomized controlled trial comparing the Coordinated Anxiety Learning and Management (CALM) intervention with UC at baseline and at 6-, 12-, and 18-month follow-up assessments.
Setting: Seventeen US primary care clinics.
Patients: Referred primary care sample, 1004 patients, with principal DSM-IV diagnoses of GAD (n = 549), PD (n = 262), SAD (n = 132), or PTSD (n = 61) (mean [SD] age, 43.7 [13.7] years; 70.9% were female). Eighty percent of the participants completed 18-month follow-up.
Interventions: CALM (cognitive behavior therapy and pharmacotherapy recommendations) and UC.
Main outcome measures: Generalized Anxiety Disorder Severity Scale, Panic Disorder Severity-Self-report Scale, Social Phobia Inventory, and PTSD Checklist-Civilian Version scores.
Results: CALM was superior to UC for principal GAD at 6-month (-1.61; 95% confidence interval [CI], -2.42 to -0.79), 12-month (-2.34; -3.22 to -1.45), and 18-month (-2.37; -3.24 to -1.50), PD at 6-month (-2.00; -3.55 to -0.44) and 12-month (-2.71; -4.29 to -1.14), and SAD at 6-month (-7.05; -12.11 to -2.00) outcomes. CALM was superior to UC for comorbid SAD at 6-month (-4.26; 95% CI, -7.96 to -0.56), 12-month (-8.12, -11.84 to -4.40), and 18- month (-6.23, -9.90 to -2.55) outcomes. Effect sizes favored CALM but were not statistically significant for other comorbid disorders.
Conclusions: CALM (cognitive behavior therapy and pharmacotherapy medication recommendations) is more effective than is UC for principal anxiety disorders and, to a lesser extent, comorbid anxiety disorders that present in primary care.
Figures
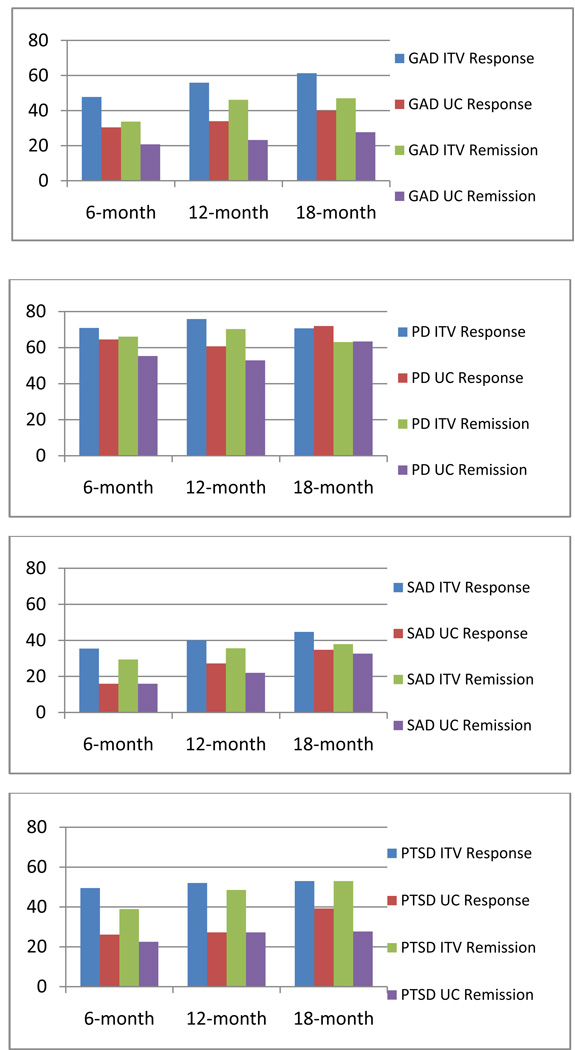
| GAD | PD |
 GAD ITV Response GAD ITV Response | PD ITV Response |
 GAD UC Response GAD UC Response | PD UC Response |
 GAD ITV Remission GAD ITV Remission | PD ITV Remission |
 GAD UC Remission GAD UC Remission | PD UC Remission |
| SAD | PTSD |
| SAD ITV Response | PTSD ITV Response |
| SAD UC Response | PTSD UC Response |
| SAD ITV Remission | PTSD ITV Remission |
| SAD UC Remission | PTSD UC Remission |
References
-
- Saarni SJ, Suvisaari J, Sintonen H, Pirkola S, Koskinen S, Aromaa A, Lonnqvist J. Impact of psychiatric disorders on health-related quality of life. Br J Psychiatry. 2005;190:326–332. - PubMed
-
- Sareen J, Jacobi F, Cox BJ, Belik SL, Clara I, Stein MB. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med. 2006;166:2109–2116. - PubMed
-
- Stein MB, Roy-Byrne PP, Craske MG, Bystritsky A, Sullivan G, Pyne JM, Wayne K, Sherbourne C. Functional Impact and Health Utility of Anxiety Disorders in Primary Care Outpatients. Medical Care. 2005;43(12):1164–1170. - PubMed
-
- Kroenke K, Spitzer RL, Williams JB, Monahan PO, Lowe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146:317–325. - PubMed
