

Efficacy of anti-inflammatory therapy in a model of acute seizures and in a population of pediatric drug resistant epileptics
- PMID: 21464890
- PMCID: PMC3065475
- DOI: 10.1371/journal.pone.0018200
Efficacy of anti-inflammatory therapy in a model of acute seizures and in a population of pediatric drug resistant epileptics
Abstract
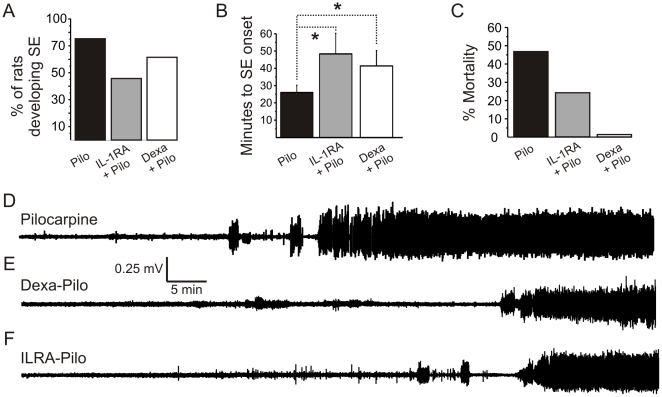
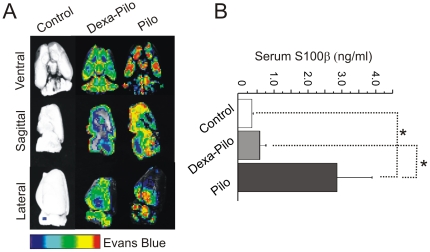
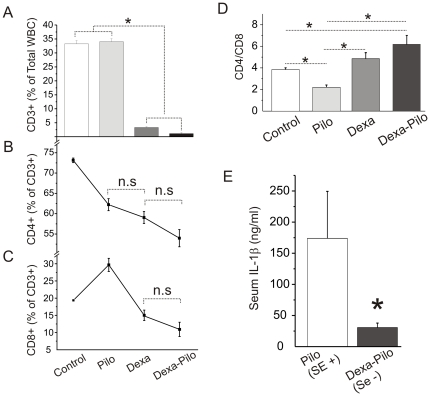
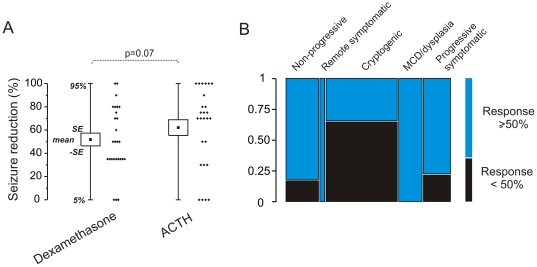
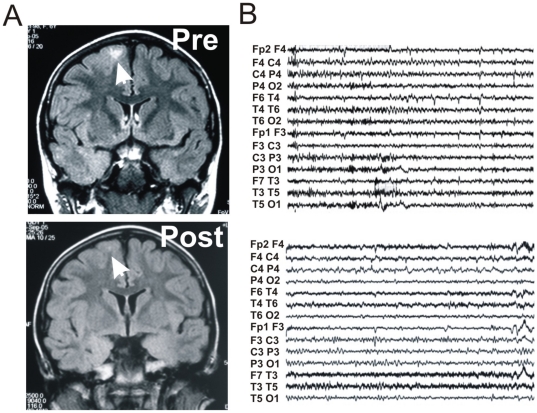
Targeting pro-inflammatory events to reduce seizures is gaining momentum. Experimentally, antagonism of inflammatory processes and of blood-brain barrier (BBB) damage has been demonstrated to be beneficial in reducing status epilepticus (SE). Clinically, a role of inflammation in the pathophysiology of drug resistant epilepsies is suspected. However, the use anti-inflammatory drug such as glucocorticosteroids (GCs) is limited to selected pediatric epileptic syndromes and spasms. Lack of animal data may be one of the reasons for the limited use of GCs in epilepsy. We evaluated the effect of the CG dexamethasone in reducing the onset and the severity of pilocarpine SE in rats. We assessed BBB integrity by measuring serum S100β and Evans Blue brain extravasation. Electrophysiological monitoring and hematologic measurements (WBCs and IL-1β) were performed. We reviewed the effect of add on dexamethasone treatment on a population of pediatric patients affected by drug resistant epilepsy. We excluded subjects affected by West, Landau-Kleffner or Lennox-Gastaut syndromes and Rasmussen encephalitis, known to respond to GCs or adrenocorticotropic hormone (ACTH). The effect of two additional GCs, methylprednisolone and hydrocortisone, was also reviewed in this population. When dexamethasone treatment preceded exposure to the convulsive agent pilocarpine, the number of rats developing status epilepticus (SE) was reduced. When SE developed, the time-to-onset was significantly delayed compared to pilocarpine alone and mortality associated with pilocarpine-SE was abolished. Dexamethasone significantly protected the BBB from damage. The clinical study included pediatric drug resistant epileptic subjects receiving add on GC treatments. Decreased seizure frequency (≥ 50%) or interruption of status epilepticus was observed in the majority of the subjects, regardless of the underlying pathology. Our experimental results point to a seizure-reducing effect of dexamethasone. The mechanism encompasses improvement of BBB integrity. Our results also suggest that add on GCs could be of efficacy in controlling pediatric drug resistant seizures.
Conflict of interest statement
Figures
References
-
- Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen HW, et al. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2009 - PubMed
-
- Elkassabany NM, Bhatia J, Deogaonkar A, Barnett GH, Lotto M, et al. Perioperative complications of blood brain barrier disruption under general anesthesia: a retrospective review. J Neurosurg Anesthesiol. 2008;20:45–48. - PubMed
-
- Korn A, Golan H, Melamed I, Pascual-Marqui R, Friedman A. Focal cortical dysfunction and blood-brain barrier disruption in patients with Postconcussion syndrome. J Clin Neurophysiol. 2005;22:1–9. - PubMed
-
- Ivens S, Kaufer D, Flores LP, Bechmann I, Zumsteg D, et al. TGF-beta receptor-mediated albumin uptake into astrocytes is involved in neocortical epileptogenesis. Brain. 2007;130:535–547. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
