

Percutaneous instrumentation of the cervical and cervico-thoracic spine using pedicle screws: preliminary clinical results and analysis of accuracy
- PMID: 21465291
- PMCID: PMC3099152
- DOI: 10.1007/s00586-011-1775-9
Percutaneous instrumentation of the cervical and cervico-thoracic spine using pedicle screws: preliminary clinical results and analysis of accuracy
Abstract
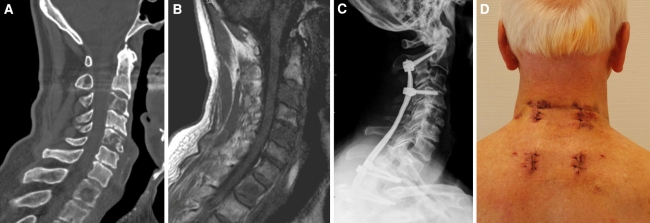
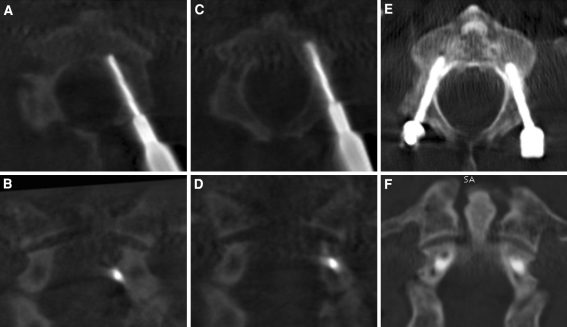
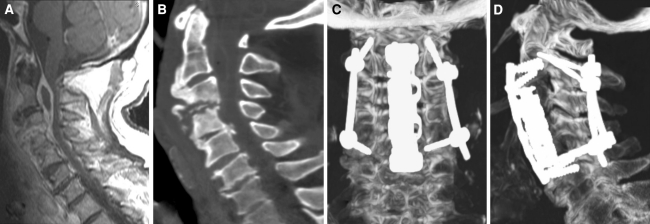
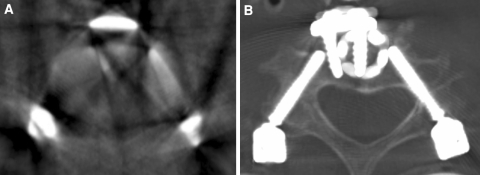
The pedicle screw instrumentation represents the most rigid construct of the cervical and cervicothoracic spine and in spite of the risks to neurovascular structures clinical relevant complications do not occur frequently. The steep angles of the cervical pedicles result in a wide surgical exposure with extensive muscular trauma. The objective of this study was the evaluation of the accuracy of cervical pedicle screw insertion through a minimally invasive technique to reduce access-related muscular trauma. Therefore, percutaneous transpedicular instrumentation of the cervical and cervicothoracic spine was performed in 15 patients using fluoroscopy. All instrumentations from C2 to Th4 were inserted bilaterally through 2 to 3-cm skin and fascia incisions even in multilevel procedures and the rods were placed by blunt insertion through the incision. Thin-cut CT scan was used postoperatively to analyze pedicle violations. 76.4% of 72 screws were placed accurately. Most pedicle perforations were seen laterally towards the vertebral artery. Critical breaches >2 mm or narrowing of the transversal foramen occurred in 12.5% of screws; however, no revision surgery for screw displacement was needed in the absence of clinical symptoms. No conversion from percutaneous to open surgery was necessary. It was concluded that percutaneous transpedicular instrumentation of the cervical spine is a surgically demanding technique and should be reserved for experienced spine surgeons. The indications are limited to instrumentation-only procedures or in combination with anterior treatment, but with the potential to minimize access-related morbidity.
Figures
Similar articles
-
Computer-assisted posterior instrumentation of the cervical and cervico-thoracic spine.Eur Spine J. 2004 Feb;13(1):50-9. doi: 10.1007/s00586-003-0604-1. Epub 2003 Nov 22. Eur Spine J. 2004. PMID: 14634850 Free PMC article. Clinical Trial.
-
Development of a new technique for pedicle screw and Magerl screw insertion using a 3-dimensional image guide.Spine (Phila Pa 1976). 2012 Nov 1;37(23):1983-8. doi: 10.1097/BRS.0b013e31825ab547. Spine (Phila Pa 1976). 2012. PMID: 22531473
-
Posterior cervicothoracic instrumentation in spine tumors.Spine (Phila Pa 1976). 2004 Jun 1;29(11):1246-53. doi: 10.1097/00007632-200406010-00015. Spine (Phila Pa 1976). 2004. PMID: 15167665
-
Reconstruction of the subaxial cervical spine using pedicle screw instrumentation.Spine (Phila Pa 1976). 2012 Mar 1;37(5):E349-56. doi: 10.1097/BRS.0b013e318239cf1f. Spine (Phila Pa 1976). 2012. PMID: 22020588 Review.
-
Comparison of two novel fluoroscopy-based stereotactic methods for cervical pedicle screw placement and review of the literature.Eur Spine J. 2008 Apr;17(4):564-75. doi: 10.1007/s00586-008-0584-2. Epub 2008 Jan 22. Eur Spine J. 2008. PMID: 18210169 Free PMC article. Review.
Cited by
-
Management of hangman's fracture with percutaneous transpedicular screw fixation.Eur Spine J. 2013 Jan;22(1):79-86. doi: 10.1007/s00586-012-2578-3. Epub 2012 Nov 19. Eur Spine J. 2013. PMID: 23161420 Free PMC article.
-
Minimally invasive treatment of the thoracic spine disease: completely percutaneous and hybrid approaches.Minim Invasive Surg. 2013;2013:508920. doi: 10.1155/2013/508920. Epub 2013 Dec 16. Minim Invasive Surg. 2013. PMID: 24455233 Free PMC article.
-
Accurate placement of cervical pedicle screws using 3D-printed navigational templates : An improved technique with continuous image registration.Orthopade. 2018 May;47(5):428-436. doi: 10.1007/s00132-017-3515-2. Orthopade. 2018. PMID: 29387914 English.
-
The Feasibility of Long-Segment Fluoroscopy-guided Percutaneous Thoracic Spine Pedicle Screw Fixation, and the Outcome at Two-year Follow-up.Malays Orthop J. 2019 Nov;13(3):39-44. doi: 10.5704/MOJ.1911.007. Malays Orthop J. 2019. PMID: 31890109 Free PMC article.
-
The role of cervical pedicle screw in cervical spine trauma: A single-center retrospective study.J Craniovertebr Junction Spine. 2023 Jul-Sep;14(3):299-305. doi: 10.4103/jcvjs.jcvjs_19_23. Epub 2023 Sep 18. J Craniovertebr Junction Spine. 2023. PMID: 37860022 Free PMC article.
References
-
- Bartels E, Flugel KA. Evaluation of extracranial vertebral artery dissection with duplex color-flow imaging. Stroke. 1996;27:290–295. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
