

Nutritional phases in Prader-Willi syndrome
- PMID: 21465655
- PMCID: PMC3285445
- DOI: 10.1002/ajmg.a.33951
Nutritional phases in Prader-Willi syndrome
Abstract
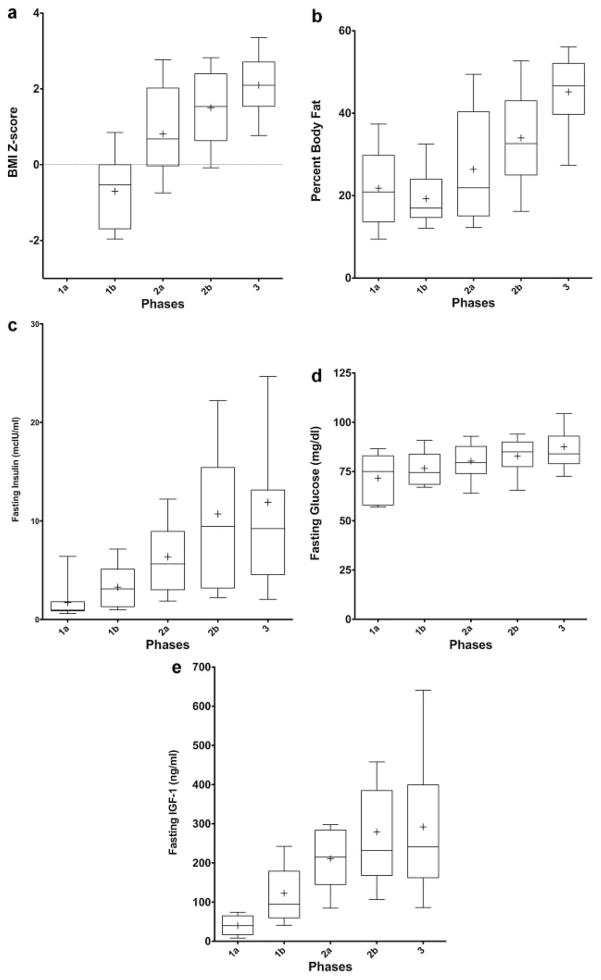
Prader-Willi syndrome (PWS) is a complex neurobehavioral condition which has been classically described as having two nutritional stages: poor feeding, frequently with failure to thrive (FTT) in infancy (Stage 1), followed by hyperphagia leading to obesity in later childhood (Stage 2). We have longitudinally followed the feeding behaviors of individuals with PWS and found a much more gradual and complex progression of the nutritional phases than the traditional two stages described in the literature. Therefore, this study characterizes the growth, metabolic, and laboratory changes associated with the various nutritional phases of PWS in a large cohort of subjects. We have identified a total of seven different nutritional phases, with five main phases and sub-phases in phases 1 and 2. Phase 0 occurs in utero, with decreased fetal movements and growth restriction compared to unaffected siblings. In phase 1 the infant is hypotonic and not obese, with sub-phase 1a characterized by difficulty feeding with or without FTT (ages birth-15 months; median age at completion: 9 months). This phase is followed by sub-phase 1b when the infant grows steadily along a growth curve and weight is increasing at a normal rate (median age of onset: 9 months; age quartiles 5-15 months). Phase 2 is associated with weight gain-in sub-phase 2a the weight increases without a significant change in appetite or caloric intake (median age of onset 2.08 years; age quartiles 20-31 months;), while in sub-phase 2b the weight gain is associated with a concomitant increased interest in food (median age of onset: 4.5 years; quartiles 3-5.25 years). Phase 3 is characterized by hyperphagia, typically accompanied by food-seeking and lack of satiety (median age of onset: 8 years; quartiles 5-13 years). Some adults progress to phase 4 which is when an individual who was previously in phase 3 no longer has an insatiable appetite and is able to feel full. Therefore, the progression of the nutritional phases in PWS is much more complex than previously recognized. Awareness of the various phases will aid researchers in unraveling the pathophysiology of each phase and provide a foundation for developing rational therapies. Counseling parents of newly diagnosed infants with PWS as to what to expect with regard to these nutritional phases may help prevent or slow the early-onset of obesity in this syndrome.
Copyright © 2011 Wiley-Liss, Inc.
Figures
Comment in
-
Energy homeostasis in Prader-Willi syndrome: how clinical research informs studies of animal models of genetic obesity: comment on "Nutritional phases in Prader-Willi syndrome," Miller et al., 2011. Am J Med Genet Part A, 155:1040-1049.Am J Med Genet A. 2012 Apr;158A(4):966-8. doi: 10.1002/ajmg.a.35249. Epub 2012 Mar 14. Am J Med Genet A. 2012. PMID: 22419655 No abstract available.
References
-
- Bizzarri C, Rigamonti AE, Luce A, Cappa M, Cella SG, Berini J, Sartorio A, Muller EE, Salvatoni A. Children with Prader-Willi syndrome exhibit more evident meal-induced responses in plasma ghrelin and peptide YY levels than obese and lean children. Eur J Endocrinol. 2010;162:499–505. - PubMed
-
- Burman P, Ritzén EM, Lindgren AC. Endocrine dysfunction in Prader-Willi syndrome: A review with special reference to GH. Endocr Rev. 2001;22:787–799. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
