

Relationships among insulin resistance, type 2 diabetes, essential hypertension, and cardiovascular disease: similarities and differences
- PMID: 21466618
- PMCID: PMC8673405
- DOI: 10.1111/j.1751-7176.2011.00439.x
Relationships among insulin resistance, type 2 diabetes, essential hypertension, and cardiovascular disease: similarities and differences
Abstract
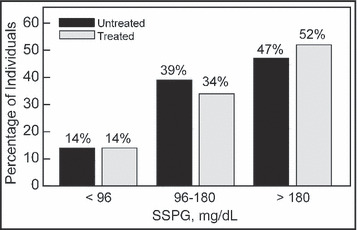
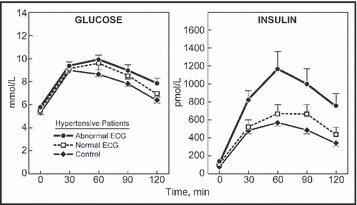
Insulin resistance plays a major role in the pathogenesis and clinical course of patients with type 2 diabetes (2DM) and essential hypertension. However, the syndromes differ in prevalence of insulin resistance, and associated insulin secretory response. Essentially all patients with type 2 diabetes are insulin resistant, whereas only approximately 50% of those with essential hypertension are insulin resistant. Furthermore, 2DM develops when the pancreatic β-cell can no longer maintain the degree of compensatory hyperinsulinemia needed to prevent hyperglycemia. In contrast, the compensatory hyperinsulinemia that prevents most insulin resistant individuals from developing 2DM acts on normally insulin sensitive tissues in a manner that predisposes to the development of essential hypertension. This review will discuss these similarities and differences in some detail, as well as exploring the relationship among insulin resistance and related metabolic abnormalities in the pathogenesis of cardiovascular disease in patients with 2DM and essential hypertension.
© 2011 Wiley Periodicals, Inc.
Figures
References
-
- Yeni‐Komshian H, Carantoni M, Abbasi F, et al. Relationship between several surrogate estimates of insulin resistance and quantification of insulin‐mediated glucose disposal in 490 healthy, nondiabetic volunteers. Diabetes Care. 2000;23:71–175. - PubMed
-
- Bogardus C, Lillioja S, Mott DM, et al. Relationship between degree of obesity and in vivo insulin action in man. Am J Physiol. 1985;248(Endocrinol Metab 11):E286–E291. - PubMed
-
- Lillioja S, Mott DM, Zawadzki J, et al. In vivo insulin action is a familial characteristic in nondiabetic Pima Indians. Diabetes. 1987;36:1329–1335. - PubMed
-
- Zoratti R, Godsland IF, Chaturvedi N, et al. Relation of plasma lipids to insulin resistance, nonesterified fatty acids, and body fat in men from three ethnic groups: relevance to variations in risk of diabetes and coronary artery disease. Metabolism. 2000;49:245–252. - PubMed
-
- Reaven G. Role of insulin resistance in human disease. Diabetes. 1988;37:1595–1607. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
