

Low-frequency HIV-1 drug resistance mutations and risk of NNRTI-based antiretroviral treatment failure: a systematic review and pooled analysis
- PMID: 21467286
- PMCID: PMC3325645
- DOI: 10.1001/jama.2011.375
Low-frequency HIV-1 drug resistance mutations and risk of NNRTI-based antiretroviral treatment failure: a systematic review and pooled analysis
Abstract
Context: Presence of low-frequency, or minority, human immunodeficiency virus type 1 (HIV-1) drug resistance mutations may adversely affect response to antiretroviral treatment (ART), but evidence regarding the effects of such mutations on the effectiveness of first-line ART is conflicting.
Objective: To evaluate the association of preexisting drug-resistant HIV-1 minority variants with risk of first-line nonnucleoside reverse transcriptase inhibitor (NNRTI)-based antiretroviral virologic failure.
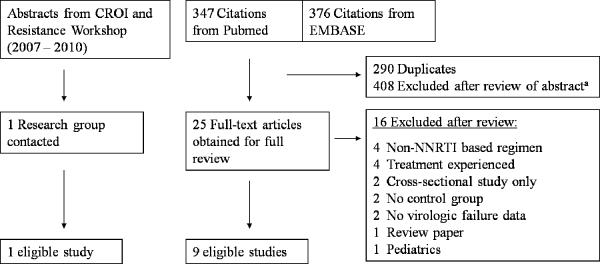
Data sources: Systematic review of published and unpublished studies in PubMed (1966 through December 2010), EMBASE (1974 through December 2010), conference abstracts, and article references. Authors of all studies were contacted for detailed laboratory, ART, and adherence data.
Study selection and data abstraction: Studies involving ART-naive participants initiating NNRTI-based regimens were included. Participants were included if all drugs in their ART regimen were fully active by standard HIV drug resistance testing. Cox proportional hazard models using pooled patient-level data were used to estimate the risk of virologic failure based on a Prentice weighted case-cohort analysis stratified by study.
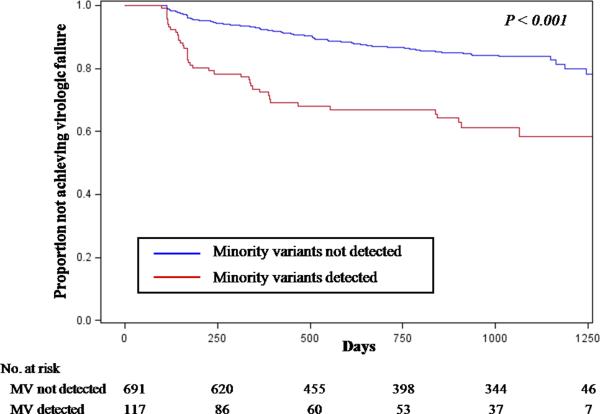
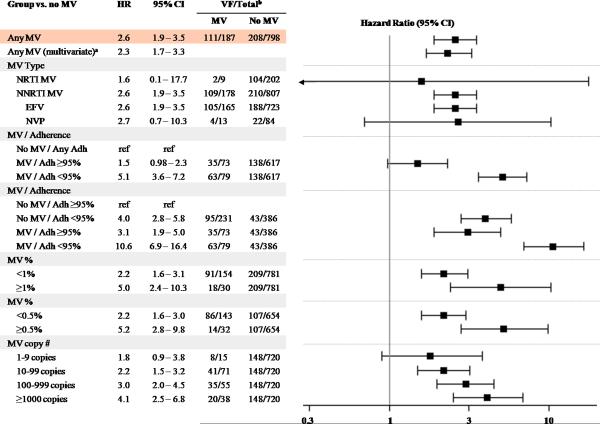
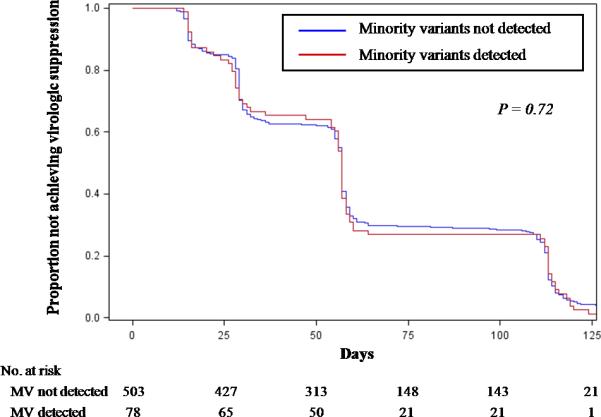
Data synthesis: Individual data from 10 studies and 985 participants were available for the primary analysis. Low-frequency drug resistance mutations were detected in 187 participants, including 117 of 808 patients in the cohort studies. Low-frequency HIV-1 drug resistance mutations were associated with an increased risk of virologic failure (hazard ratio (HR], 2.3 [95% confidence interval {CI}, 1.7-3.3]; P < .001) after controlling for medication adherence, race/ethnicity, baseline CD4 cell count, and plasma HIV-1 RNA levels. Increased risk of virologic failure was most strongly associated with minority variants resistant to NNRTIs (HR, 2.6 [95% CI, 1.9-3.5]; P < .001). Among participants from the cohort studies, 35% of those with detectable minority variants experienced virologic failure compared with 15% of those without minority variants. The presence of minority variants was associated with 2.5 to 3 times the risk of virologic failure at either 95% or greater or less than 95% overall medication adherence. A dose-dependent increased risk of virologic failure was found in participants with a higher proportion or quantity of drug-resistant variants.
Conclusion: In a pooled analysis, low-frequency HIV-1 drug resistance mutations, particularly involving NNRTI resistance, were significantly associated with a dose-dependent increased risk of virologic failure with first-line ART.
Figures
References
-
- Kim D, Wheeler W, Ziebell R, et al. Prevalence of transmitted antiretroviral drug resistance among newly-diagnosed HIV-1-infected persons, US, 2007. Paper presented at: 17th Conference on Retroviruses and Opportunistic Infections; San Francisco, CA. February 16–19, 2010.
-
- Vercauteren J, Wensing AM, van de Vijver DA, et al. Transmission of drug-resistant HIV-1 is stabilizing in Europe. J Infect Dis. 2009 Nov 15;200(10):1503–1508. - PubMed
-
- Metzner KJ, Bonhoeffer S, Fischer M, et al. Emergence of minor populations of human immunodeficiency virus type 1 carrying the M184V and L90M mutations in subjects undergoing structured treatment interruptions. J Infect Dis. 2003 Nov 15;188(10):1433–1443. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
