

Continuous femoral versus posterior lumbar plexus nerve blocks for analgesia after hip arthroplasty: a randomized, controlled study
- PMID: 21467563
- PMCID: PMC3132825
- DOI: 10.1213/ANE.0b013e318212495b
Continuous femoral versus posterior lumbar plexus nerve blocks for analgesia after hip arthroplasty: a randomized, controlled study
Abstract
Background: Hip arthroplasty frequently requires potent postoperative analgesia, often provided with an epidural or posterior lumbar plexus local anesthetic infusion. However, American Society of Regional Anesthesia guidelines now recommend against epidural and continuous posterior lumbar plexus blocks during administration of various perioperative anticoagulants often administered after hip arthroplasty. A continuous femoral nerve block is a possible analgesic alternative, but whether it provides comparable analgesia to a continuous posterior lumbar plexus block after hip arthroplasty remains unclear. We therefore tested the hypothesis that differing the catheter insertion site (femoral versus posterior lumbar plexus) after hip arthroplasty has no impact on postoperative analgesia.
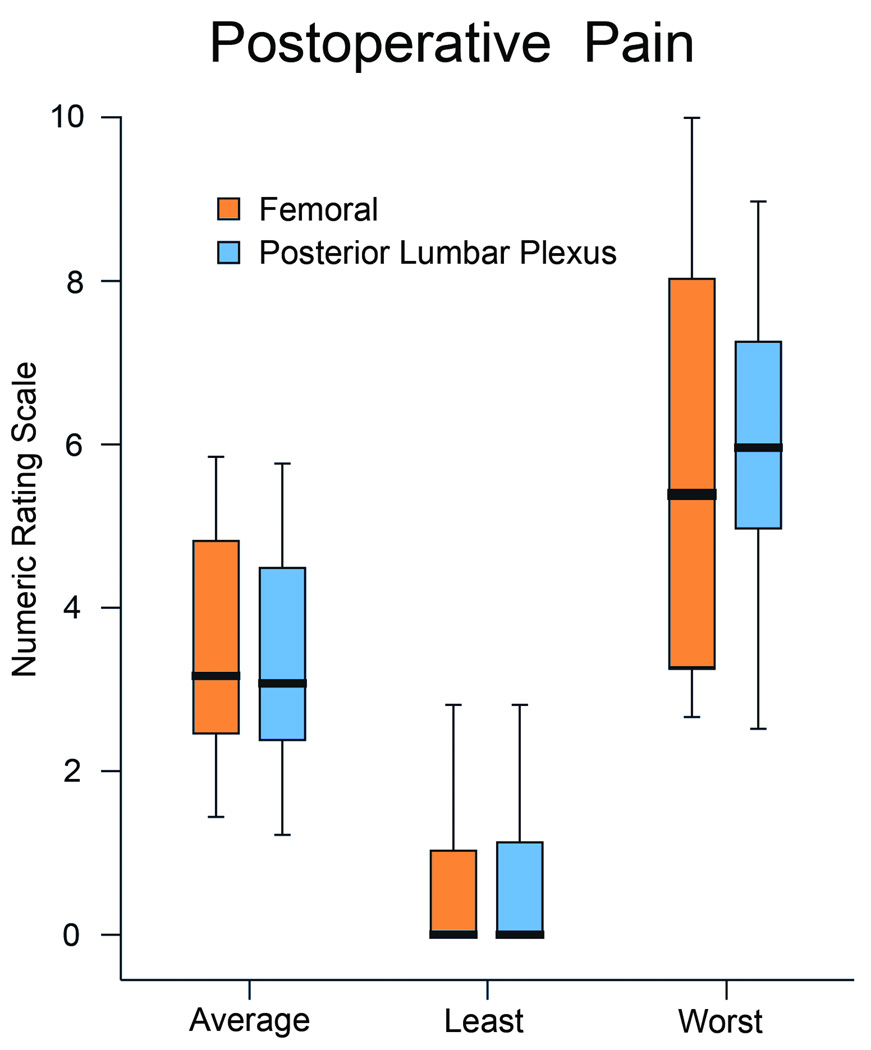
Methods: Preoperatively, subjects undergoing hip arthroplasty were randomly assigned to receive either a femoral or a posterior lumbar plexus stimulating catheter inserted 5 to 15 cm or 0 to 1 cm past the needle tip, respectively. Postoperatively, patients received perineural ropivacaine, 0.2% (basal 6 mL/hr, bolus 4 mL, 30-minute lockout) for at least 2 days. The primary end point was the average daily pain scores as measured with a numeric rating scale (0-10) recorded in the 24-hour period beginning at 07:30 the morning after surgery, excluding twice-daily physical therapy sessions. Secondary end points included pain during physical therapy, ambulatory distance, and supplemental analgesic requirements during the same 24-hour period, as well as satisfaction with analgesia during hospitalization.
Results: The mean (SD) pain scores for subjects receiving a femoral infusion (n = 25) were 3.6 (1.8) versus 3.5 (1.8) for patients receiving a posterior lumbar plexus infusion (n = 22), resulting in a group difference of 0.1 (95% confidence interval -0.9 to 1.2; P = 0.78). Because the confidence interval was within a prespecified -1.6 to 1.6 range, we conclude that the effect of the 2 analgesic techniques on postoperative pain was equivalent. Similarly, we detected no differences between the 2 treatments with respect to the secondary end points, with one exception: subjects with a femoral catheter ambulated a median (10th-90th percentiles) 2 (0-17) m the morning after surgery, in comparison with 11 (0-31) m for subjects with a posterior lumbar plexus catheter (data nonparametric; P = 0.02).
Conclusions: After hip arthroplasty, a continuous femoral nerve block is an acceptable analgesic alternative to a continuous posterior lumbar plexus block when using a stimulating perineural catheter. However, early ambulatory ability suffers with a femoral infusion.
Trial registration: ClinicalTrials.gov NCT00967980.
Conflict of interest statement
Conflict of Interest: See Disclosures at the end of the article
Figures
Comment in
-
Analgesic techniques after total hip arthroplasty.Anesth Analg. 2011 Oct;113(4):687-8. doi: 10.1213/ANE.0b013e31821aa46a. Epub 2011 Apr 25. Anesth Analg. 2011. PMID: 21519045 No abstract available.
References
-
- Buckenmaier CC, III, Xenos JS, Nilsen SM. Lumbar plexus block with perineural catheter and sciatic nerve block for total hip arthroplasty. J Arthroplasty. 2002;17:499–502. - PubMed
-
- Ilfeld BM, Ball ST, Gearen PF, Le LT, Mariano ER, Vandenborne K, Duncan PW, Sessler DI, Enneking FK, Shuster JJ, Theriaque DW, Meyer RS. Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial. Anesthesiology. 2008;109:491–501. - PMC - PubMed
-
- Ilfeld BM, Moeller LK, Mariano ER, Loland VJ, Stevens-Lapsley JE, Fleisher AS, Girard PJ, Donohue MC, Ferguson EJ, Ball ST. Continuous Peripheral Nerve Blocks: Is Local Anesthetic Dose the Only factor, or Do Concentration and volume Influence Infusion Effects as Well? Anesthesiology. 2010;112:347–354. - PubMed
-
- Capdevila X, Macaire P, Dadure C, Choquet O, Biboulet P, Ryckwaert Y, d’Athis F. Continuous psoas compartment block for postoperative analgesia after total hip arthroplasty: New landmarks, technical guidelines, and clinical evaluation. Anesth Analg. 2002;94:1606–1613. - PubMed
-
- Siddiqui ZI, Cepeda MS, Denman W, Schumann R, Carr DB. Continuous lumbar plexus block provides improved analgesia with fewer side effects compared with systemic opioids after hip arthroplasty: a randomized controlled trial. Reg Anesth Pain Med. 2007;32:393–398. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
