

Feasibility and yield of screening in relatives from familial pancreatic cancer families
- PMID: 21468009
- PMCID: PMC3683863
- DOI: 10.1038/ajg.2011.65
Feasibility and yield of screening in relatives from familial pancreatic cancer families
Abstract
Objectives: Pancreatic adenocarcinoma is a lethal disease. Over 80% of patients are found to have metastatic disease at the time of diagnosis. Strategies to improve disease-specific outcome include identification and early detection of precursor lesions or early cancers in high-risk groups. In this study, we investigate whether screening at-risk relatives of familial pancreatic cancer (FPC) patients is safe and has significant yield.
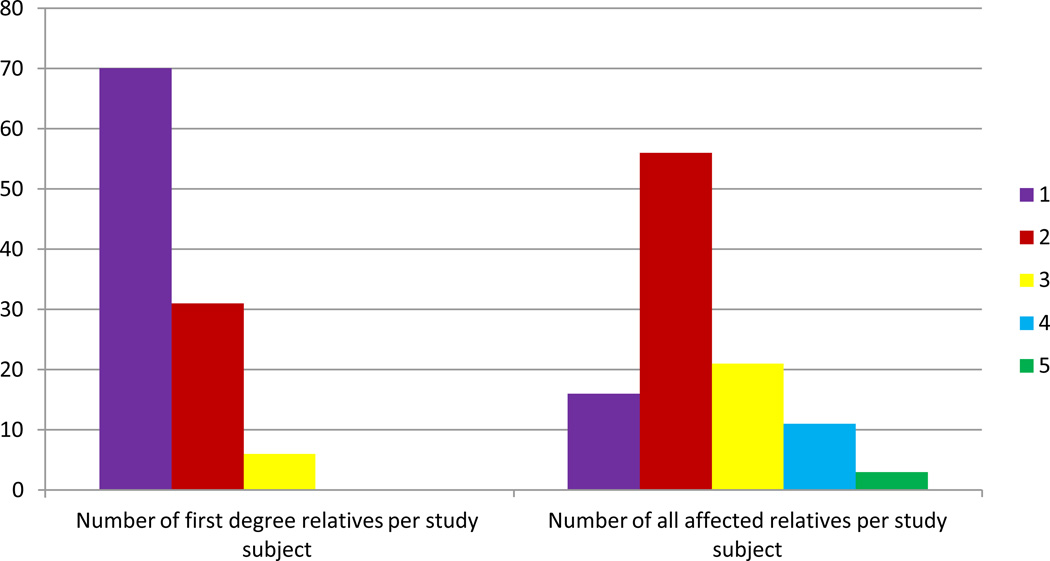
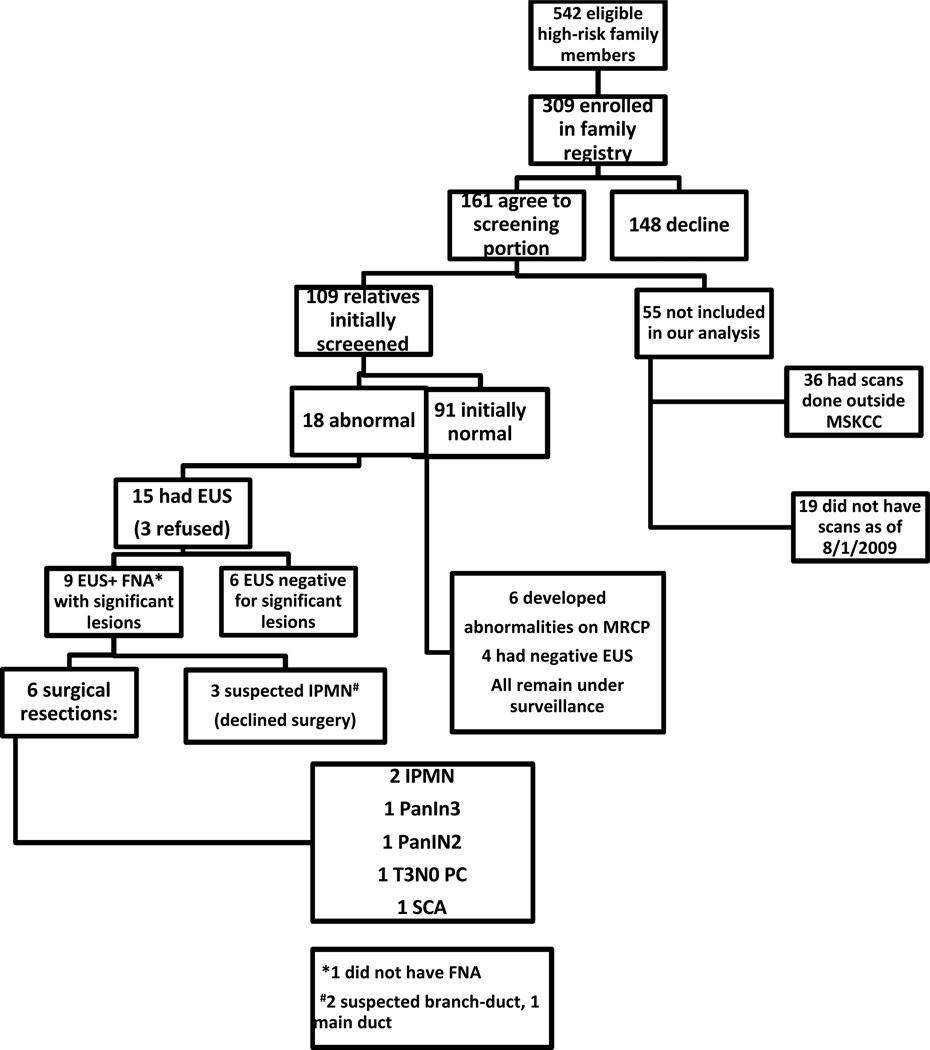
Methods: We enrolled 309 asymptomatic at-risk relatives into our Familial Pancreatic Tumor Registry (FPTR) and offered them screening with magnetic resonance cholangiopancreaticogram (MRCP) followed by endoscopic ultrasound (EUS) with fine needle aspiration if indicated. Relatives with findings were referred for surgical evaluation.
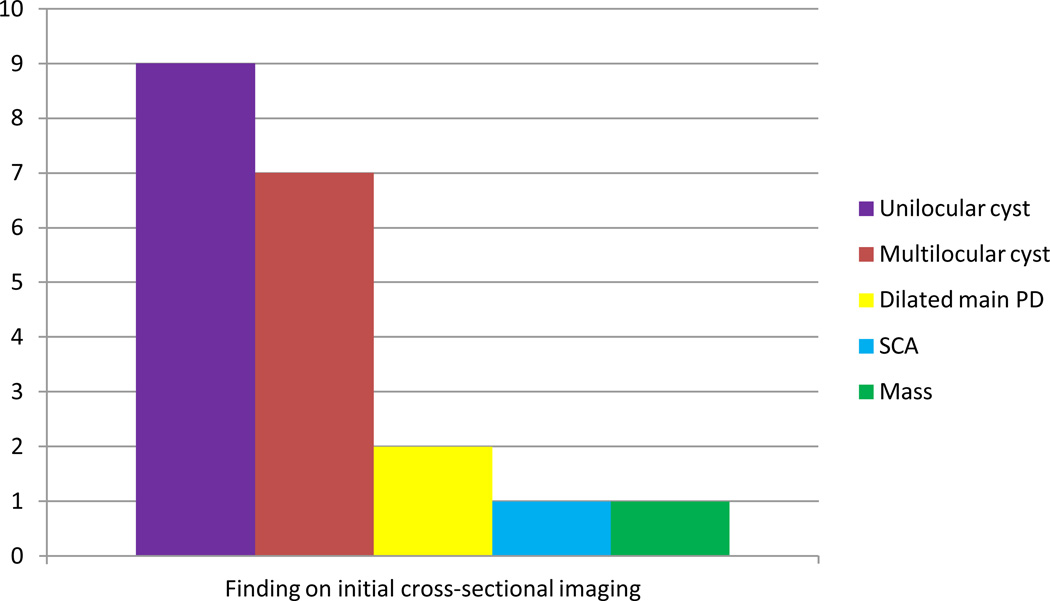
Results: As of 1 August 2009, 109 relatives had completed at least one cycle of screening. Abnormal radiographic findings were present on initial screening in 18/109 patients (16.5%), 15 of whom underwent EUS. A significant abnormality was confirmed in 9 of 15 patients, 6 of whom ultimately had surgery for an overall diagnostic yield of 8.3% (9/109). Yield was greatest in relatives >65 years old (35%, 6/17) when compared with relatives 55-65 years (3%, 1/31) and relatives <55 years (3%, 2/61).
Conclusions: Screening at-risk relatives from FPC families has a significant diagnostic yield, particularly in relatives >65 years of age, confirming prior studies. MRCP as initial screening modality is safe and effective.
Conflict of interest statement
Figures

Comment in
-
Pancreatic cancer surveillance: learning as we go.Am J Gastroenterol. 2011 May;106(5):955-6. doi: 10.1038/ajg.2011.68. Am J Gastroenterol. 2011. PMID: 21540900
References
-
- [accessed May 5, 2009];American Cancer Society. web site, www.cancer.org/downloads/STT/500809 web.pdf http://www.cancer.org/docroot/stt/stt_0.asp?from=fast.
-
- Allen PJ. Pancreatic adenocarcinoma: putting a hump in survival. J Am Coll Surg. 2007;205(4S):S76–S80. - PubMed
-
- Ries LAG, Melbert D, Krapcho M, et al., editors. SEER Cancer Statistics Review, 1975–2004. Bethesda, MD: National Cancer Institute; 2007. accessed at www.seer.cancer.gov/csr/1975_2004/
-
- Shimizu Y, Yasui K, Matsueda K, et al. Small carcinoma of the pancreas is curable: new computed tomography finding, pathological study and postoperative results from a single institute. J Gastroenterol Hepatol. 2005;20(10):1591–1594. - PubMed
-
- Ahlgren JD. Epidemiology and risk factors in pancreatic cancer. Semin Oncol. 1996;23:241–250. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
