

Cost effectiveness of outpatient treatment for febrile neutropaenia in adult cancer patients
- PMID: 21468048
- PMCID: PMC3101923
- DOI: 10.1038/bjc.2011.101
Cost effectiveness of outpatient treatment for febrile neutropaenia in adult cancer patients
Abstract
Background: There is uncertainty whether low-risk episodes of febrile neutropaenia (FN) in adult cancer patients are best managed in the in- or outpatient setting.
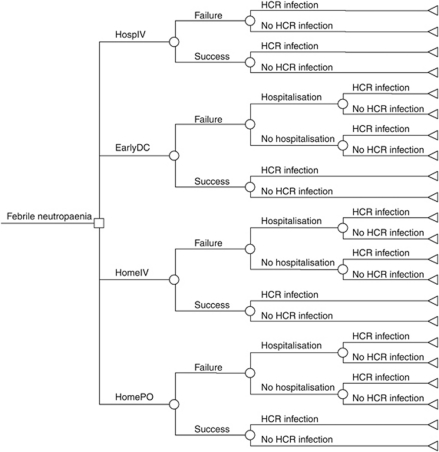
Methods: A Monte Carlo cost-utility model was created to compare four treatment strategies for low-risk FN: (1) treatment in hospital with intravenous antibiotics (HospIV); (2) early discharge after 48 h in-patient observation, followed by oral outpatient treatment (EarlyDC); (3) outpatient management with IV antibiotics (HomeIV); and (4) outpatient management with oral antibiotics (HomePO). The model used a health-care payer perspective and a time horizon of one FN episode. Outcome measures were quality-adjusted FN episodes (QAFNE), costs (Canadian dollars) and incremental cost-effectiveness ratios (ICER). Parameter uncertainty was assessed with probabilistic sensitivity analyses.
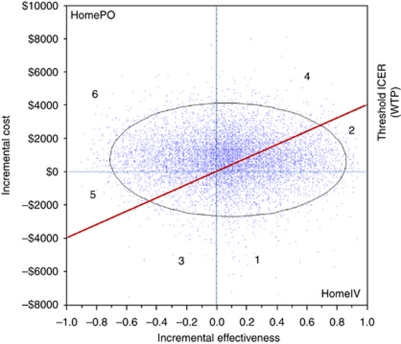
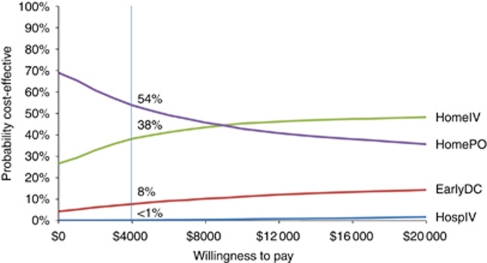
Results: HomePO was cost saving ($3470 vs $4183), but less effective (0.65 QAFNE vs 0.72 QAFNE) than HomeIV. The corresponding ICER was $10,186 per QAFNE. Both EarlyDC ($6115; 0.66 QAFNE) and HospIV ($13,557; 0.62 QAFNE) were dominated strategies. At a willingness-to-pay (WTP) threshold of $4,000 per QAFNE, HomePO and HomeIV were cost effective in 54 and 38% of simulations, respectively.
Interpretation: For adult cancer patients with an episode of low-risk FN, treatment in hospital is more expensive and less effective than outpatient strategies.
Figures
References
-
- Bala MV, Zarkin GA (2000) Are QALYs an appropriate measure for valuing morbidity in acute diseases? Health Econ 9: 177–180 - PubMed
-
- Bennett CL, Calhoun EA (2007) Evaluating the total costs of chemotherapy-induced febrile neutropenia: results from a pilot study with community oncology cancer patients. Oncologist 12: 478–483 - PubMed
-
- Birch S, Gafni A (2006) Information created to evade reality (ICER): things we should not look to for answers. Pharmacoeconomics 24: 1121–1131 - PubMed
-
- Brown RE, Hutton J, Burrell A (2001) Cost effectiveness of treatment options in advanced breast cancer in the UK. Pharmacoeconomics 19: 1091–1102 - PubMed
-
- Chamilos G, Bamias A, Efstathiou E, Zorzou PM, Kastritis E, Kostis E, Papadimitriou C, Dimopoulos MA (2005) Outpatient treatment of low-risk neutropenic fever in cancer patients using oral moxifloxacin. Cancer 103: 2629–2635 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
