

Clinical effectiveness of the Respimat inhaler device in managing chronic obstructive pulmonary disease: evidence when compared with other handheld inhaler devices
- PMID: 21468167
- PMCID: PMC3064421
- DOI: 10.2147/COPD.S8092
Clinical effectiveness of the Respimat inhaler device in managing chronic obstructive pulmonary disease: evidence when compared with other handheld inhaler devices
Abstract
Objectives: Medication for the management of chronic obstructive pulmonary disease (COPD) may be delivered by a number of different inhaler devices. This study was undertaken to determine the clinical effectiveness of the Respimat handheld inhaler device compared with other handheld inhaler devices for the delivery of medication in stable COPD.
Methodology: A systematic review of high-quality randomized controlled clinical trials comparing Respimat with other inhaler devices using the same medication was performed. Studies were searched for in the Cochrane Central Register of Controlled Trials as well as other relevant electronic databases. Manufacturers of inhaled COPD medication were also contacted for potential trials.
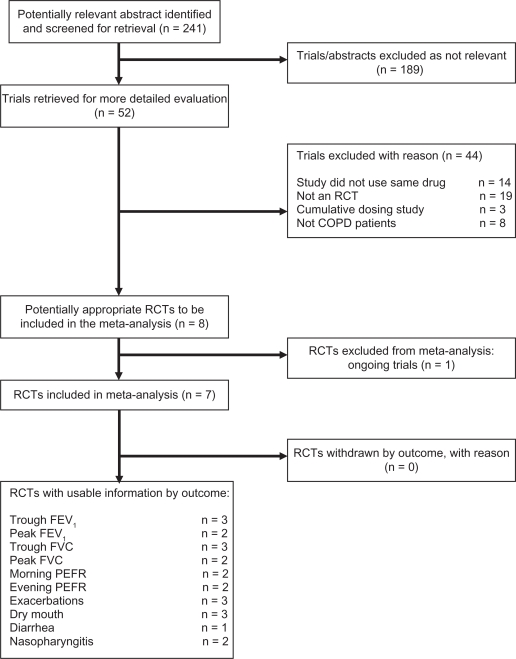
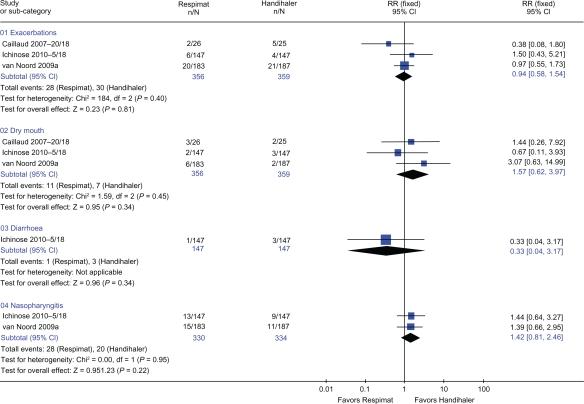
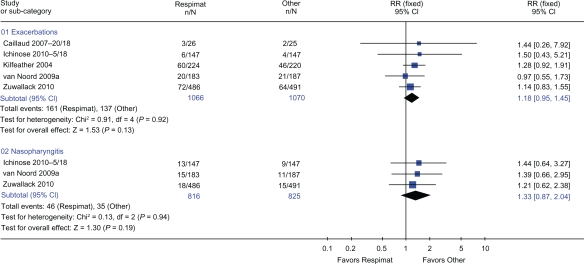
Results: Seven studies of high methodological quality with 3813 participants were included in the review. Three trials used Handihaler as the comparator inhaler, three used a chlorofluorocarbon metered-dose inhaler (CFC-MDI), and one trial used a hydroflouroalkane (HFA)-MDI. When Respimat was compared with Handihaler, the following reported outcomes were not significantly different: trough forced expiratory volume in 1 second (FEV(1)) (weighted mean difference [WMD] 0.01 L; P = 0.14), trough forced vital capacity (FVC) (WMD 0.001 L: P = 0.88), peak FEV(1) (WMD 0.01 L: P = 0.08), peak FVC (WMD 0.01 L: P = 0.55), morning peak expiratory flow rate (PEFR) (WMD 5.06 L/min: P = 0.08), and evening PEFR (WMD 4.39 L/min: P = 0.15). Furthermore, there were no differences when Respimat was compared with Handihaler for risk of exacerbations (relative risk [RR] 0.94: P = 0.81), dry mouth (RR 1.57: P = 0.34), or nasopharyngitis (RR 1.42: P = 0.22). For Respimat compared with CFC-MDI, the only outcome for which data were available for meta-analysis was exacerbations, which were not significantly different (RR 1.20: P = 0.12). In addition, five trials with 2136 patients showed that there was no difference in risk of exacerbations or nasopharyngitis when Respimat was compared with all other handheld inhaler devices (RR 1.18: P = 0.13 and RR 1.33: P = 0.19, respectively). None of the clinical outcome measures reported was significantly different when the same, higher, or lower doses of medication were used in the inhaler devices being compared. Unfortunately, none of the included trials reported mortality as an outcome measure.
Conclusions: Evidence from high-quality trials published to date suggests that the Respimat inhaler does not provide any additional clinical benefit to that provided by other inhaler devices in the management of COPD. Although in vitro studies have reported differences between the Respimat inhaler device and other handheld devices, we found no difference in any clinical outcome measures, including lung function and adverse events. Although recent reports have highlighted concerns of increased mortality with the Respimat inhaler device, none of the included trials reported mortality as an outcome. Only a small number of trials reported data that could be used in this systematic review, and a limited number of studies have been published that compare Respimat with other inhaler devices using the same drug and strength. Therefore, further trials comparing Respimat with other handheld inhaler devices using the same drug and dose are required before firm conclusions can be drawn. The concern with increased mortality with Respimat use should be investigated urgently.
Keywords: COPD; Respimat; aerosol cloud; handheld inhaler devices.
Figures


References
-
- Schurmann W, Schmidtmann S, Moroni P, et al. Respimat Soft Mist inhaler versus hydrofluoroalkane metered dose inhaler: patient preference and satisfaction. Treat Respir Med. 2005;4(1):53–61. - PubMed
-
- Dalby R, Spallek M, Voshaar T. A review of the development of Respimat® Soft Mist™ Inhaler. Int J Pharm. 2004;283(1–2):1–9. - PubMed
-
- Spallek M, Hochrainer D, Wachtel H. Optimizing nozzles for soft mist inhalers. Respiratory Drug Delivery. 2002;VIII(2):375–378.
-
- Hochrainer D, Holz H, Kreher C, et al. Comparison of the aerosol velocity and spray duration of Respimat® Soft Mist™ inhaler and pressurized metered dose inhalers. J Aerosol Med. 2005;18(3):273–282. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
