

Barriers to adherence to chronic obstructive pulmonary disease guidelines by primary care physicians
- PMID: 21468169
- PMCID: PMC3064423
- DOI: 10.2147/COPD.S16396
Barriers to adherence to chronic obstructive pulmonary disease guidelines by primary care physicians
Abstract
Purpose: Even with the dissemination of several clinical guidelines, chronic obstructive pulmonary disease (COPD) remains underdiagnosed and mismanaged by many primary care physicians (PCPs). The objective of this study was to elucidate barriers to consistent implementation of COPD guidelines.
Patients and methods: A cross-sectional study implemented in July 2008 was designed to assess attitudes and barriers to COPD guideline usage.
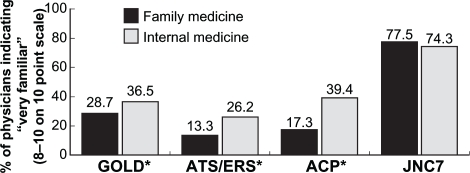
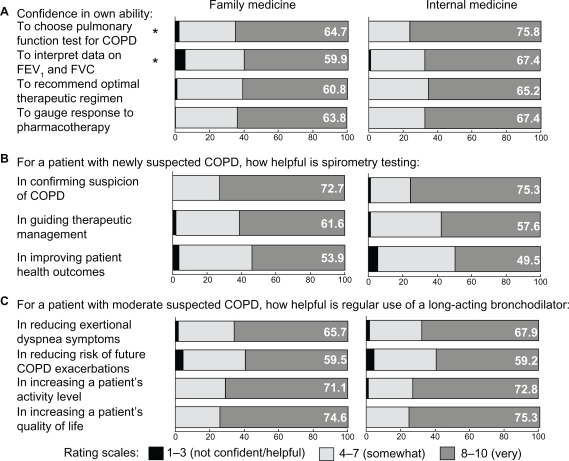
Results: Five hundred US PCPs (309 family medicine physicians, 191 internists) were included in the analysis. Overall, 23.6% of the surveyed PCPs reported adherence to spirometry guidelines over 90% of the time; 25.8% reported adherence to guidelines related to long-acting bronchodilator (LABD) use in COPD patients. In general, physicians were only somewhat familiar with COPD guidelines, and internal medicine physicians were significantly more familiar than family physicians (P < 0.05). In a multivariate model controlling for demographics and barriers to guideline adherence, we found significant associations with two tested guideline components. Adherence to spirometry guidelines was associated with agreement with guidelines, confidence in interpreting data, ambivalence to outcome expectancy, and ability to incorporate spirometry into patient flow. Adherence to LABD therapy guidelines was associated with agreement with guidelines and confidence in gauging pharmacologic response.
Conclusions: Adherence to guideline recommendations of spirometry use was predicted by agreement with the recommendations, self-efficacy, perceived outcome expectancy if recommendations were adhered to, and resource availability. Adherence to recommendations of LABD use was predicted by agreement with guideline recommendations and self-efficacy. Increasing guideline familiarity alone may have limited patient outcomes, as other barriers, such as low confidence and outcome expectancy, are more likely to impact guideline adherence.
Keywords: COPD; barriers; guideline adoption; primary care.
Figures
Similar articles
-
Continuing to Confront COPD International Physician Survey: physician knowledge and application of COPD management guidelines in 12 countries.Int J Chron Obstruct Pulmon Dis. 2014 Dec 30;10:39-55. doi: 10.2147/COPD.S70162. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2014. PMID: 25565799 Free PMC article.
-
Guideline-based COPD management in a resource-limited setting - physicians' understanding, adherence and barriers: a cross-sectional survey of internal and family medicine hospital-based physicians in Nigeria.Prim Care Respir J. 2013 Mar;22(1):79-85. doi: 10.4104/pcrj.2013.00014. Prim Care Respir J. 2013. PMID: 23443222 Free PMC article.
-
Guideline-based survey of outpatient COPD management by pulmonary specialists in Germany.Int J Chron Obstruct Pulmon Dis. 2012;7:101-8. doi: 10.2147/COPD.S27887. Epub 2012 Feb 14. Int J Chron Obstruct Pulmon Dis. 2012. PMID: 22371651 Free PMC article.
-
Review: clinical inertia in the management of chronic obstructive pulmonary disease.COPD. 2012 Feb;9(1):73-80. doi: 10.3109/15412555.2011.631957. COPD. 2012. PMID: 22292599 Review.
-
A review of the GOLD guidelines for the diagnosis and treatment of patients with COPD.Int J Clin Pract. 2008 Aug;62(8):1219-36. doi: 10.1111/j.1742-1241.2008.01807.x. Epub 2008 Jun 28. Int J Clin Pract. 2008. PMID: 18547365 Review.
Cited by
-
[Perceptions of patients and health professionals about the quality of care provided to chronic obstructive pulmonary disease patients].Aten Primaria. 2016 Feb;48(2):85-94. doi: 10.1016/j.aprim.2015.02.011. Epub 2015 May 19. Aten Primaria. 2016. PMID: 26002749 Free PMC article. Spanish.
-
Distribution, Temporal Stability and Appropriateness of Therapy of Patients With COPD in the UK in Relation to GOLD 2019.EClinicalMedicine. 2019 Jul 24;14:32-41. doi: 10.1016/j.eclinm.2019.07.003. eCollection 2019 Sep. EClinicalMedicine. 2019. PMID: 31709400 Free PMC article.
-
Primary care COPD patients compared with large pharmaceutically-sponsored COPD studies: an UNLOCK validation study.PLoS One. 2014 Mar 5;9(3):e90145. doi: 10.1371/journal.pone.0090145. eCollection 2014. PLoS One. 2014. PMID: 24598945 Free PMC article.
-
Compliance of Pharmacotherapy with GOLD Guidelines: A Longitudinal Study in Patients with COPD.Int J Chron Obstruct Pulmon Dis. 2020 Mar 26;15:627-635. doi: 10.2147/COPD.S240444. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32273691 Free PMC article.
-
COPD management by Swedish general practitioners - baseline results of the PRIMAIR study.Scand J Prim Health Care. 2018 Mar;36(1):5-13. doi: 10.1080/02813432.2018.1426148. Epub 2018 Jan 15. Scand J Prim Health Care. 2018. PMID: 29334861 Free PMC article.
References
-
- Barr RG, Celli BR, Martinez FJ, et al. Physician and patient perceptions in COPD: the COPD Resource Network Needs Assessment Survey. Am J Med. 2005;118(12):1415. - PubMed
-
- Pierson DJ. Clinical practice guidelines for chronic obstructive pulmonary disease: a review and comparison of current resources. Respir Care. 2006;51(3):277–288. - PubMed
-
- Tinkelman DG, Price DB, Nordyke RJ, Halbert RJ. Misdiagnosis of COPD and asthma in primary care patients 40 years of age and over. J Asthma. 2006;43(1):75–80. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
