

Maternal health-related quality of life after induction of labor or expectant monitoring in pregnancy complicated by intrauterine growth retardation beyond 36 weeks
- PMID: 21468753
- PMCID: PMC3195683
- DOI: 10.1007/s11136-011-9891-x
Maternal health-related quality of life after induction of labor or expectant monitoring in pregnancy complicated by intrauterine growth retardation beyond 36 weeks
Abstract
Objective: Pregnancies complicated by intrauterine growth retardation (IUGR) beyond 36 weeks of gestation are at increased risk of neonatal morbidity and mortality. Optimal treatment in IUGR at term is highly debated. Results from the multicenter DIGITAT (Disproportionate Intrauterine Growth Intervention Trial At Term) trial show that induction of labor and expectant monitoring result in equal neonatal and maternal outcomes for comparable cesarean section rates. We report the maternal health-related quality of life (HR-QoL) that was measured alongside the trial at several points in time.
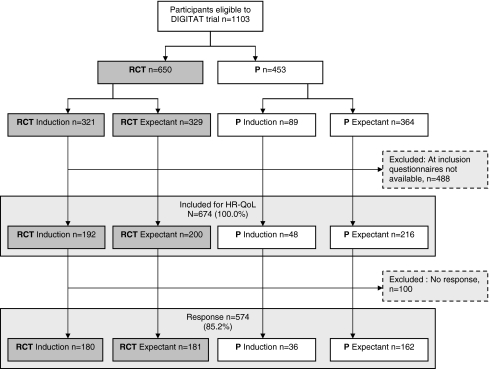
Methods: Both randomized and non-randomized women were asked to participate in the HR-QoL study. Women were asked to fill out written validated questionnaires, covering background characteristics, condition-specific issues and the Short Form (SF-36), European Quality of Life (EuroQoL 6D3L), Hospital Anxiety and Depression scale (HADS), and Symptom Check List (SCL-90) at baseline, 6 weeks postpartum and 6 months postpartum. We compared the difference scores of all summary measures between the two management strategies by ANOVA. A repeated measures multivariate mixed model was defined to assess the effect of the management strategies on the physical (PCS) and mental (MCS) components of the SF-36. Analysis was by intention to treat.
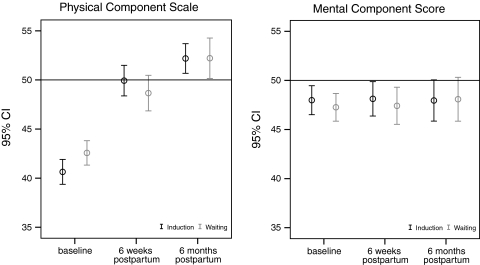
Results: We analyzed data of 361 randomized and 198 non-randomized patients. There were no clinically relevant differences between the treatments at 6 weeks or 6 months postpartum on any summary measures; e.g., on the SF-36 (PCS: P = .09; MCS: P = .48). The PCS and the MCS were below norm values at inclusion. The PCS improved over time but stayed below norm values at 6 months, while the MCS did not improve.
Conclusion: In pregnancies complicated by IUGR beyond 36 weeks, induction of labor does not affect the long-term maternal quality of life.
Figures
References
-
- Dijxhoorn MJ, Visser GH, Touwen BC, Huisjes HJ. Apgar score, meconium and acidaemia at birth in small-for-gestational age infants born at term, and their relation to neonatal neurological morbidity. British Journal of Obstetrics and Gynaecology. 1987;94(9):873–879. doi: 10.1111/j.1471-0528.1987.tb03758.x. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
