

What is the most accurate whole-body imaging modality for assessment of local and distant recurrent disease in colorectal cancer? A meta-analysis : imaging for recurrent colorectal cancer
- PMID: 21468765
- PMCID: PMC3126998
- DOI: 10.1007/s00259-011-1785-1
What is the most accurate whole-body imaging modality for assessment of local and distant recurrent disease in colorectal cancer? A meta-analysis : imaging for recurrent colorectal cancer
Abstract
Purpose: The objective of this study was to compare the diagnostic performance of positron emission tomography (PET), PET/CT, CT and MRI as whole-body imaging modalities for the detection of local and/or distant recurrent disease in colorectal cancer (CRC) patients who have a (high) suspicion of recurrent disease, based on clinical findings or rise in carcinoembryonic antigen (CEA).
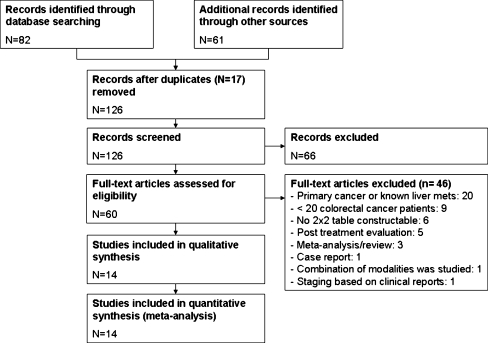
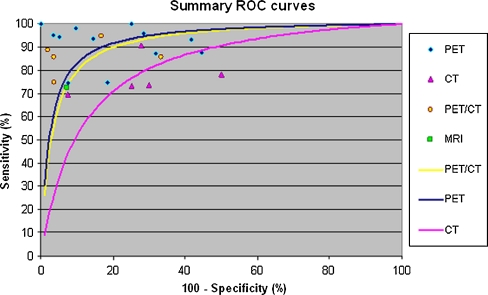
Methods: A meta-analysis was undertaken. PubMed and Embase were searched for studies on the accuracy of whole-body imaging for patients with suspected local and/or distant recurrence of their CRC. Additionally, studies had to have included at least 20 patients with CRC and 2 × 2 contingency tables had to be provided or derivable. Articles evaluating only local recurrence or liver metastasis were excluded. Summary receiver-operating characteristic (ROC) curves were constructed from the data on sensitivity and specificity of individual studies and pooled estimates of diagnostic odds ratios (DORs) and areas under the ROC curve (AUCs) were calculated. To test for heterogeneity the Cochran Q test was used.
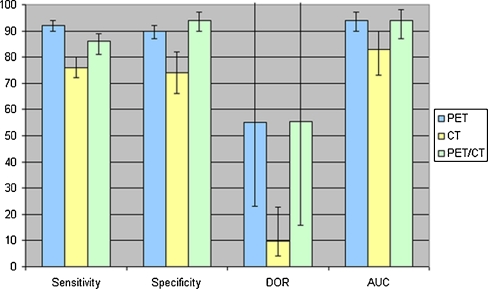
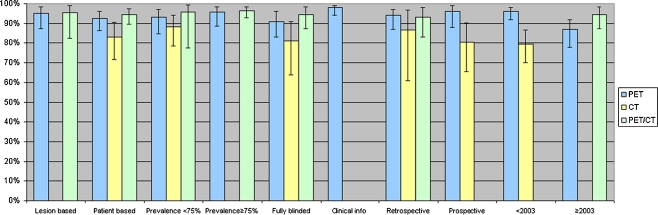
Results: Fourteen observational studies were included which evaluated PET, PET/CT, CT and/or MRI. Study results were available in 12 studies for PET, in 5 studies for CT, in 5 studies for PET/CT and in 1 study for MRI. AUCs for PET, PET/CT and CT were 0.94 (0.90-0.97), 0.94 (0.87-0.98) and 0.83 (0.72-0.90), respectively. In patient based analyses PET/CT had a higher diagnostic performance than PET with an AUC of 0.95 (0.89-0.97) for PET/CT vs 0.92 (0.86-0.96) for PET.
Conclusion: Both whole-body PET and PET/CT are very accurate for the detection of local and/or distant recurrent disease in CRC patients with a (high) suspicion of recurrent disease. CT has the lowest diagnostic performance. This difference is probably mainly due to the lower accuracy of CT for detection of extrahepatic metastases (including local recurrence). For clinical practice PET/CT might be the modality of choice when evaluating patients with a (high) suspicion of recurrent disease, because of its best performance in patient based analyses and confident prediction of disease status.
Figures

Similar articles
-
Whole-body MRI at 1.5 T and 3 T compared with FDG-PET-CT for the detection of tumour recurrence in patients with colorectal cancer.Eur Radiol. 2009 Jun;19(6):1366-78. doi: 10.1007/s00330-008-1289-y. Epub 2009 Feb 4. Eur Radiol. 2009. PMID: 19190917
-
A two-way comparison of whole-body 18FDG PET-CT and whole-body contrast-enhanced MRI for distant metastasis staging in patients with malignant tumors: a meta-analysis of 13 prospective studies.Ann Palliat Med. 2020 Mar;9(2):247-255. doi: 10.21037/apm.2020.02.30. Epub 2020 Mar 18. Ann Palliat Med. 2020. PMID: 32233618 Review.
-
Diagnostic Value of (18)F-FDG PET/CT in Detecting Local Recurrent Colorectal Cancer: A Pooled Analysis of 26 Individual Studies.Cell Biochem Biophys. 2015 Jun;72(2):443-51. doi: 10.1007/s12013-014-0485-4. Cell Biochem Biophys. 2015. PMID: 25737131
-
18F-FDG PET/CT and whole-body MRI diagnostic performance in M staging for non-small cell lung cancer: a systematic review and meta-analysis.Eur Radiol. 2020 Jul;30(7):3641-3649. doi: 10.1007/s00330-020-06703-1. Epub 2020 Mar 3. Eur Radiol. 2020. PMID: 32125513
-
Prospective study on diagnostic and prognostic significance of postoperative FDG PET/CT in recurrent colorectal carcinoma patients: comparison with MRI and tumor markers.Neoplasma. 2017;64(6):954-961. doi: 10.4149/neo_2017_613. Neoplasma. 2017. PMID: 28895416
Cited by
-
Surveillance Intensity Comparison by Risk for T1NX Locally Excised Rectal Adenocarcinoma: a Cost-Effective Analysis.J Gastrointest Surg. 2020 Jan;24(1):198-208. doi: 10.1007/s11605-019-04369-9. Epub 2019 Nov 13. J Gastrointest Surg. 2020. PMID: 31724115
-
Non-invasive diagnostic imaging of colorectal liver metastases.World J Radiol. 2015 Jul 28;7(7):157-69. doi: 10.4329/wjr.v7.i7.157. World J Radiol. 2015. PMID: 26217455 Free PMC article. Review.
-
[Importance of FDG-PET/computed tomography in colorectal cancer].Radiologe. 2019 Sep;59(9):812-819. doi: 10.1007/s00117-019-00584-2. Radiologe. 2019. PMID: 31428810 Review. German.
-
Surveillance strategies following curative resection and non-operative approach of rectal cancer: How and how long? Review of current recommendations.World J Gastrointest Surg. 2023 Feb 27;15(2):177-192. doi: 10.4240/wjgs.v15.i2.177. World J Gastrointest Surg. 2023. PMID: 36896297 Free PMC article. Review.
-
Imaging in the era of risk-adapted treatment in colon cancer.Br J Radiol. 2024 Jun 18;97(1159):1214-1221. doi: 10.1093/bjr/tqae061. Br J Radiol. 2024. PMID: 38648743 Free PMC article. Review.
References
-
- Cancer Research UK. http://www.cancerresearchuk.org/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
