

Shedding of pandemic (H1N1) 2009 virus among health care personnel, Seattle, Washington, USA
- PMID: 21470453
- PMCID: PMC3377395
- DOI: 10.3201/eid1704.100866
Shedding of pandemic (H1N1) 2009 virus among health care personnel, Seattle, Washington, USA
Abstract
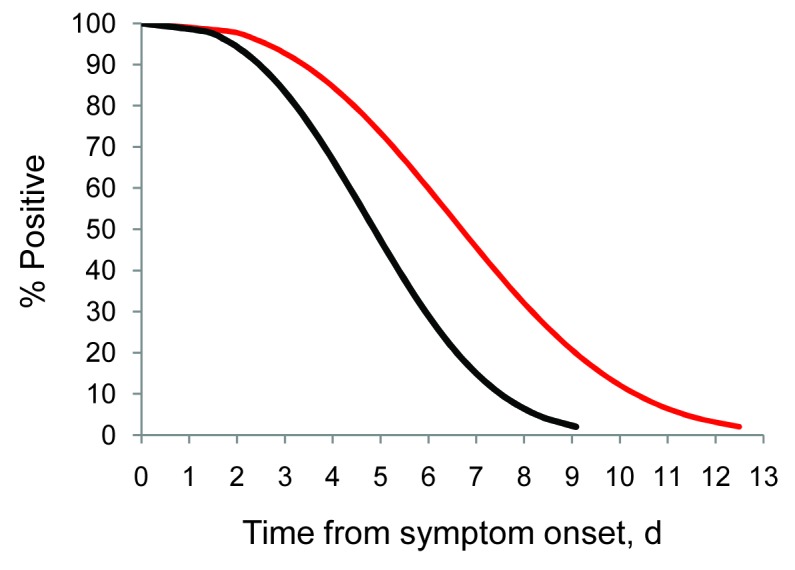
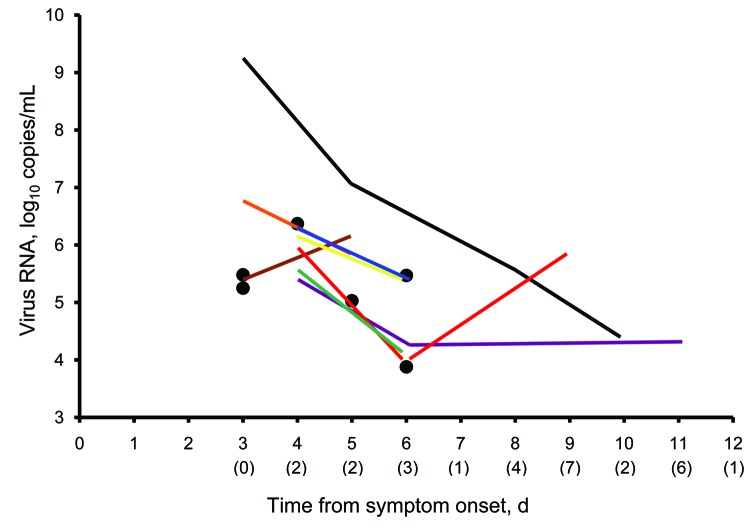
The Centers for Disease Control and Prevention (CDC) recommends that health care personnel (HCP) infected with pandemic influenza (H1N1) 2009 virus not work until 24 hours after fever subsides without the use of antipyretics. During an influenza outbreak, we examined the association between viral shedding and fever among infected HCP. Participants recorded temperatures daily and provided nasal wash specimens for 2 weeks after symptom onset. Specimens were tested by using PCR and culture. When they met CDC criteria for returning to work, 12 of 16 HCP (75%) (95% confidence interval 48%-93%) had virus detected by PCR, and 9 (56%) (95% confidence interval 30%-80%) had virus detected by culture. Fever was not associated with shedding duration (p = 0.65). HCP might shed virus even when meeting CDC exclusion guidelines. Further research is needed to clarify the association between viral shedding, symptoms, and infectiousness.
Figures
Similar articles
-
Factors promoting the prolonged shedding of the pandemic (H1N1) 2009 influenza virus in patients treated with oseltamivir for 5 days.Influenza Other Respir Viruses. 2013 Sep;7(5):833-7. doi: 10.1111/irv.12065. Epub 2012 Dec 26. Influenza Other Respir Viruses. 2013. PMID: 23279949 Free PMC article.
-
Effects of early oseltamivir therapy on viral shedding in 2009 pandemic influenza A (H1N1) virus infection.Clin Infect Dis. 2010 Apr 1;50(7):963-9. doi: 10.1086/651083. Clin Infect Dis. 2010. PMID: 20180701
-
Effectiveness of oseltamivir on disease progression and viral RNA shedding in patients with mild pandemic 2009 influenza A H1N1: opportunistic retrospective study of medical charts in China.BMJ. 2010 Sep 28;341:c4779. doi: 10.1136/bmj.c4779. BMJ. 2010. PMID: 20876641 Free PMC article.
-
Heterogeneity in transmissibility and shedding SARS-CoV-2 via droplets and aerosols.Elife. 2021 Apr 16;10:e65774. doi: 10.7554/eLife.65774. Elife. 2021. PMID: 33861198 Free PMC article.
-
An influenza A H1N1 virus revival - pandemic H1N1/09 virus.Infection. 2009 Oct;37(5):381-9. doi: 10.1007/s15010-009-9181-5. Epub 2009 Sep 18. Infection. 2009. PMID: 19768379 Review.
Cited by
-
A rapid evidence appraisal of influenza vaccination in health workers: An important policy in an area of imperfect evidence.Vaccine X. 2019 Jul 11;2:100036. doi: 10.1016/j.jvacx.2019.100036. eCollection 2019 Aug 9. Vaccine X. 2019. PMID: 31384750 Free PMC article. Review.
-
Lessons from a one-year hospital-based surveillance of acute respiratory infections in Berlin- comparing case definitions to monitor influenza.BMC Public Health. 2012 Mar 27;12:245. doi: 10.1186/1471-2458-12-245. BMC Public Health. 2012. PMID: 22452874 Free PMC article.
-
Predictors of influenza a molecular viral shedding in Hutterite communities.Influenza Other Respir Viruses. 2017 May;11(3):254-262. doi: 10.1111/irv.12448. Epub 2017 Mar 16. Influenza Other Respir Viruses. 2017. PMID: 28207989 Free PMC article.
-
Economic consequences of Japanese schools' recovery certificate policy for seasonal influenza.BMC Public Health. 2019 Mar 8;19(1):280. doi: 10.1186/s12889-019-6600-0. BMC Public Health. 2019. PMID: 30849942 Free PMC article.
-
Systematic review of influenza A(H1N1)pdm09 virus shedding: duration is affected by severity, but not age.Influenza Other Respir Viruses. 2014 Mar;8(2):142-50. doi: 10.1111/irv.12216. Epub 2013 Dec 2. Influenza Other Respir Viruses. 2014. PMID: 24299099 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Interim guidance on infection control measures for 2009. H1N1 influenza in healthcare settings, including protection of healthcare personnel [cited 2010 Dec 21]. http://www.cdc.gov/h1n1flu/guidelines_infection_control.htm
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous