

Management of recurrent post-prostatectomy incontinence after previous failed retrourethral male slings
- PMID: 21470536
- PMCID: PMC3104426
- DOI: 10.5489/cuaj.10092
Management of recurrent post-prostatectomy incontinence after previous failed retrourethral male slings
Abstract
Objective: Our objective was to establish the feasibility of combining 2 minimally invasive procedures in patients with failed primary treatment (male sling) in post-prostatectomy incontinence (PPI) patients.
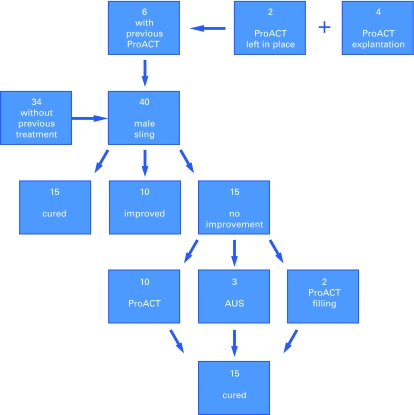
Methods: From January 2007 to July 2008, 40 men with PPI were implanted with a suburethral tape (2 patients with Seratim, 3 with I-Stop and 35 with Advance). The median preoperative pad count was 4 (range 2-10). Prior to sling placement, 6 patients had undergone ProACT implantation. Of these, 4 patients required explantation due to balloon migration and 2 patients had their balloons kept in situ, with the balloons deflated.
Results: Twenty-five patients were socially continent at this time. Fifteen patients (37.5%) did not improve or their improvement was not significant. These patients had a preoperative pad count between 7 and 10. Two of these patients had prostate adjustable continence therapy (ProACT) systems still in place. By gradually filling the balloons to 3 mL, both of these patients achieved complete continence, which was maintained at a mean follow-up of 8.5 months. Three patients with prior pelvic irradiation received an artificial urinary sphincter and achieved continence at mean follow-up of 8.3 months. The remaining 10 patients received a ProACT system in addition to the already implanted sling. After appropriate healing and filling of the balloons (average balloon volume 5 mL), all 10 patients reached complete continence; they were pad-free at a mean follow-up of 6 months (range 3-9).
Conclusions: The combination of ProACT and a suburethral tape was demonstrated to be a possible treatment option in recurrent or persistent PPI.
Objectif :: Notre objectif était d’établir la faisabilité d’une association de 2 interventions minimalement invasives chez des patients ayant subi un échec thérapeutique primaire (bandelettes sous-urétrales) chez des patients atteints d’incontinence post-prostatectomie.
Méthodologie :: De janvier 2007 à juillet 2008, on a placé une bandelette sous-urétrale chez 40 hommes atteints d’incontinence post-prostatectomie (2 patients ont reçu le dispositif de marque Seratim, 3 patients, de marque I-Stop et 35, de marque Advance). Le nombre médian de protections absorbantes avant l’opération était de 4 (2 à 10). Avant la mise en place de la bandelette, 6 patients avaient subi une implantation d’un système ProACT. De ce nombre, 4 patients ont dû se faire retirer les ballonnets en raison de leur déplacement; chez 2 patients, les ballonnets sont restés en place mais se sont dégonflés.
Résultats :: Vingt-cinq patients présentaient une continence sociale à ce moment. Quinze patients (37,5 %) n’ont présenté aucune amélioration, ou une amélioration non significative. Ces patients utilisaient de 7 à 10 protections absorbantes avant l’opération. Deux de ces patients étaient toujours porteurs d’un système ProACT. En remplissant graduellement les ballonnets de 3 mL, ces deux patients ont atteint une continence totale, maintenue après un suivi moyen de 8,5 mois. Trois patients ayant reçu antérieurement un traitement pelvien par rayonnement ont reçu un sphincter urinaire artificiel et ont atteint la continence après un suivi moyen de 8,3 mois. Chez les 10 derniers patients, on a implanté un système ProACT en plus de la bandelette déjà en place. Après un temps suffisant de guérison et le remplissage des ballonnets (volume moyen : 5 mL), les 10 patients ont atteint une continence complète. Ils n’avaient plus besoin de protection absorbante après un suivi moyen de 6 mois (entre 3 et 9 mois).
Conclusions :: L’association d’un système ProACT et d’une bandelette sous-urétrale s’est révélée une option thérapeutique possible en présence d’incontinence post-prostatectomie récurrente ou persistante.
Figures
Comment in
-
Combination options with the male urethral sling to treating post-prostatectomy incontinence.Can Urol Assoc J. 2011 Apr;5(2):112. doi: 10.5489/cuaj.11051. Can Urol Assoc J. 2011. PMID: 21470537 Free PMC article. No abstract available.
References
-
- Augustin H, Pummer K, Daghofer F, et al. Patient self-reporting questionnaire on urological morbidity and bother after radical retropubic prostatectomy. Eur Urol. 2002;42:112–7. - PubMed
-
- Burkhard FC, Kessler TM, Fleischmann A, et al. Nerve-sparing open radical retropubic prostatectomy—does it have an impact on urinary continence? J Urol. 2006;176:189–95. - PubMed
-
- Penson DF, McLerran D, Feng Z, et al. Five-year urinary and sexual outcomes after radical prostatectomy: results from the prostate cancer outcomes study. J Urol. 2005;173:1701–5. - PubMed
-
- Rudy DC, Woodside JR, Crawford ED. Urodynamic evaluation of incontinence in patients undergoing modified Campbell radical retropubic prostatectomy: a prospective study. J Urol. 1984;132:708–12. - PubMed
-
- Peyromaure M, Ravery V, Boccon-Gibod L. The management of stress urinary incontinence after radical prostatectomy. BJU Int. 2002;90:155–61. - PubMed
LinkOut - more resources
Full Text Sources
