

Practical method of adaptive radiotherapy for prostate cancer using real-time electromagnetic tracking
- PMID: 21470786
- PMCID: PMC3132289
- DOI: 10.1016/j.ijrobp.2011.01.040
Practical method of adaptive radiotherapy for prostate cancer using real-time electromagnetic tracking
Abstract
Purpose: We have created an automated process using real-time tracking data to evaluate the adequacy of planning target volume (PTV) margins in prostate cancer, allowing a process of adaptive radiotherapy with minimal physician workload. We present an analysis of PTV adequacy and a proposed adaptive process.
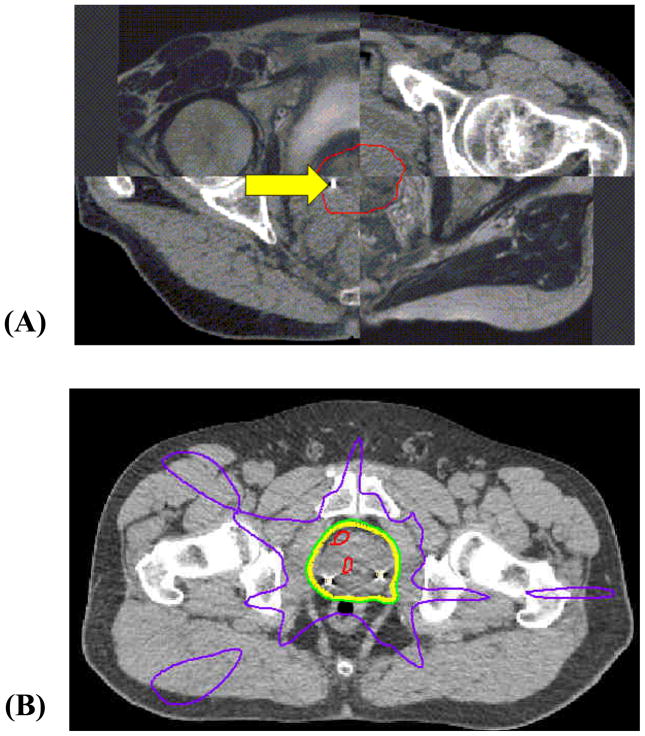
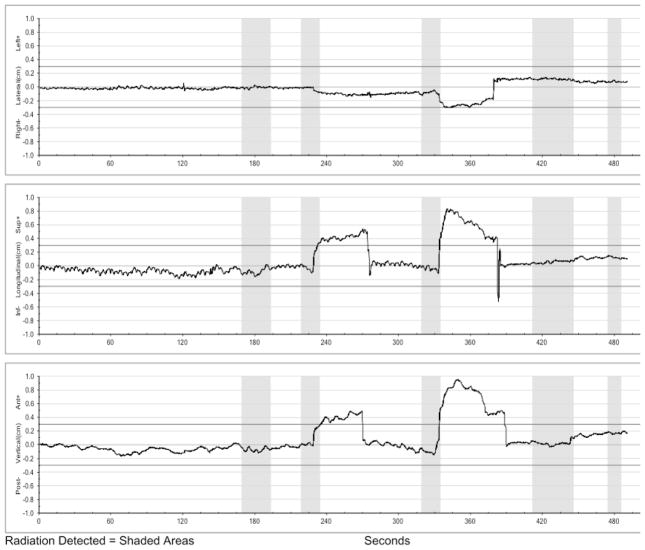
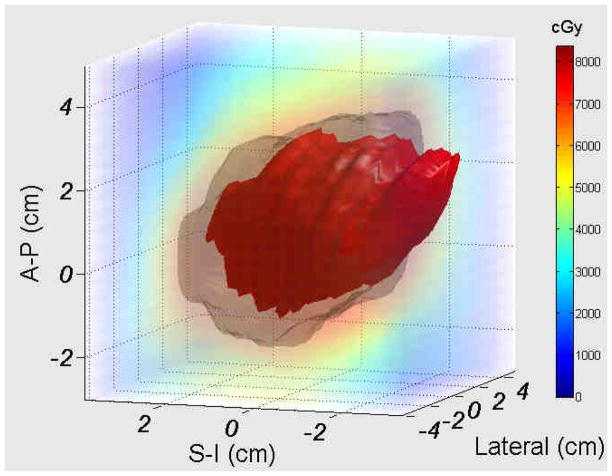
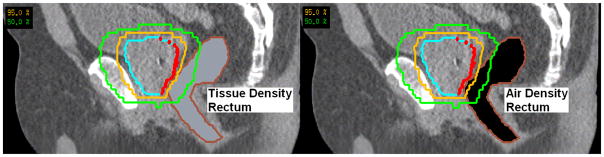
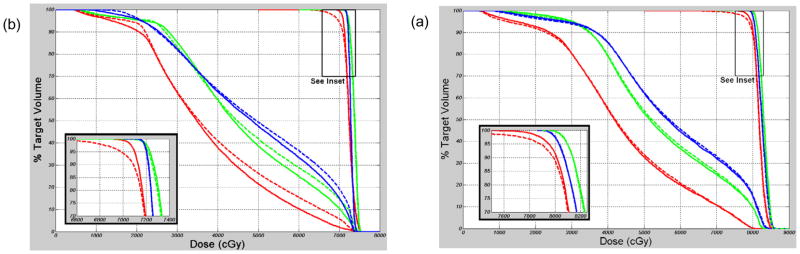
Methods and materials: Tracking data were analyzed for 15 patients who underwent step-and-shoot multi-leaf collimation (SMLC) intensity-modulated radiation therapy (IMRT) with uniform 5-mm PTV margins for prostate cancer using the Calypso® Localization System. Additional plans were generated with 0- and 3-mm margins. A custom software application using the planned dose distribution and structure location from computed tomography (CT) simulation was developed to evaluate the dosimetric impact to the target due to motion. The dose delivered to the prostate was calculated for the initial three, five, and 10 fractions, and for the entire treatment. Treatment was accepted as adequate if the minimum delivered prostate dose (D(min)) was at least 98% of the planned D(min).
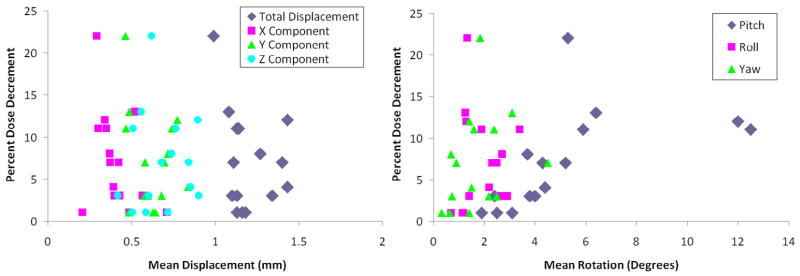
Results: For 0-, 3-, and 5-mm PTV margins, adequate treatment was obtained in 3 of 15, 12 of 15, and 15 of 15 patients, and the delivered D(min) ranged from 78% to 99%, 96% to 100%, and 99% to 100% of the planned D(min). Changes in D(min) did not correlate with magnitude of prostate motion. Treatment adequacy during the first 10 fractions predicted sufficient dose delivery for the entire treatment for all patients and margins.
Conclusions: Our adaptive process successfully used real-time tracking data to predict the need for PTV modifications, without the added burden of physician contouring and image analysis. Our methods are applicable to other uses of real-time tracking, including hypofractionated treatment.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Research interface provided by Calypso Medical Technologies. Dr. Parikh receives research funding from Calypso Medical Technologies. Supported in part by NCI R01CA134541.
Figures

Similar articles
-
Dosimetric and radiobiological consequences of computed tomography-guided adaptive strategies for intensity modulated radiation therapy of the prostate.Int J Radiat Oncol Biol Phys. 2013 Dec 1;87(5):874-80. doi: 10.1016/j.ijrobp.2013.07.006. Epub 2013 Aug 24. Int J Radiat Oncol Biol Phys. 2013. PMID: 23978708
-
Dosimetric comparison of MR-linac-based IMRT and conventional VMAT treatment plans for prostate cancer.Radiat Oncol. 2021 Jul 21;16(1):133. doi: 10.1186/s13014-021-01858-7. Radiat Oncol. 2021. PMID: 34289868 Free PMC article.
-
Dosimetric effects of adaptive prostate cancer radiotherapy in an MR-linac workflow.Radiat Oncol. 2020 Jul 10;15(1):168. doi: 10.1186/s13014-020-01604-5. Radiat Oncol. 2020. PMID: 32650811 Free PMC article.
-
Current status of intensity-modulated radiation therapy for prostate cancer: History, clinical results and future directions.Int J Urol. 2019 Aug;26(8):775-784. doi: 10.1111/iju.14011. Epub 2019 May 21. Int J Urol. 2019. PMID: 31115116 Review.
-
Magnetic Resonance Imaging-Guided Adaptive Radiation Therapy: A "Game Changer" for Prostate Treatment?Int J Radiat Oncol Biol Phys. 2018 Feb 1;100(2):361-373. doi: 10.1016/j.ijrobp.2017.10.020. Epub 2017 Oct 26. Int J Radiat Oncol Biol Phys. 2018. PMID: 29353654 Review.
Cited by
-
Motion-compensated estimation of delivered dose during external beam radiation therapy: implementation in Philips' Pinnacle(3) treatment planning system.Med Phys. 2012 Jan;39(1):437-43. doi: 10.1118/1.3670374. Med Phys. 2012. PMID: 22225314 Free PMC article.
-
Effects on the photon beam from an electromagnetic array used for patient localization and tumor tracking.J Appl Clin Med Phys. 2013 May 6;14(3):4138. doi: 10.1120/jacmp.v14i3.4138. J Appl Clin Med Phys. 2013. PMID: 23652247 Free PMC article.
-
Impact of inter- and intrafraction deviations and residual set-up errors on PTV margins. Different alignment techniques in 3D conformal prostate cancer radiotherapy.Strahlenther Onkol. 2013 Apr;189(4):321-8. doi: 10.1007/s00066-012-0303-0. Epub 2013 Feb 28. Strahlenther Onkol. 2013. PMID: 23443612
-
Evaluating the potential benefit of reduced planning target volume margins for low and intermediate risk patients with prostate cancer using real-time electromagnetic tracking.Adv Radiat Oncol. 2018 Jul 11;3(4):630-638. doi: 10.1016/j.adro.2018.06.004. eCollection 2018 Oct-Dec. Adv Radiat Oncol. 2018. PMID: 30370364 Free PMC article.
-
[Planning target volume : Management of uncertainties, immobilization, image guided and adaptive radiation therapy].Radiologe. 2018 Aug;58(8):736-745. doi: 10.1007/s00117-018-0419-z. Radiologe. 2018. PMID: 29946893 Review. German.
References
-
- Beckendorf V, Guerif S, Prise EL, et al. 70 Gy versus (vs) 80 Gy Dose Escalation Getug 06 French Trial for Localized Prostate Cancer: Mature Results. International Journal of Radiation Oncology, Biology, Physics. 2008;72:S96–97.
-
- Dearnaley DP, Sydes MR, Graham JD, et al. Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT01 randomised controlled trial. [see comment] Lancet Oncology. 2007;8:475–487. - PubMed
-
- Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. [see comment] International Journal of Radiation Oncology, Biology, Physics. 2008;70:67–74. - PubMed
-
- Peeters ST, Heemsbergen WD, Koper PC, et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. [see comment] Journal of Clinical Oncology. 2006;24:1990–1996. - PubMed
-
- Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. [see comment][erratum appears in JAMA. 2008 Feb 27;299(8):899–900] JAMA. 2005;294:1233–1239. - PubMed
