

Circulating endothelial microparticles as a measure of early lung destruction in cigarette smokers
- PMID: 21471087
- PMCID: PMC3172886
- DOI: 10.1164/rccm.201012-2061OC
Circulating endothelial microparticles as a measure of early lung destruction in cigarette smokers
Abstract
Rationale: There is increasing evidence that emphysema is associated with primary loss of pulmonary capillary endothelium. Plasma levels of endothelial microparticles (EMPs), small vesicles released from activated or apoptotic endothelial cells, are elevated in vascular-related disorders.
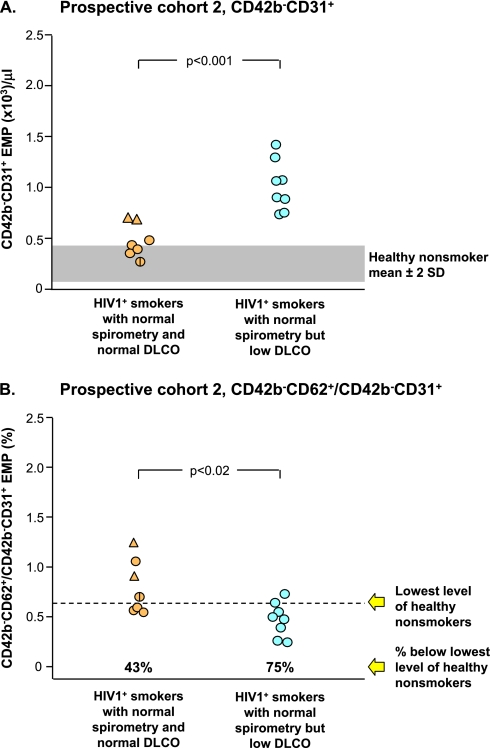
Objectives: To evaluate whether plasma EMP levels are elevated in smokers with early lung destruction as assessed by normal spirometry but reduced diffusing capacity of the lung for carbon monoxide (Dl(co)).
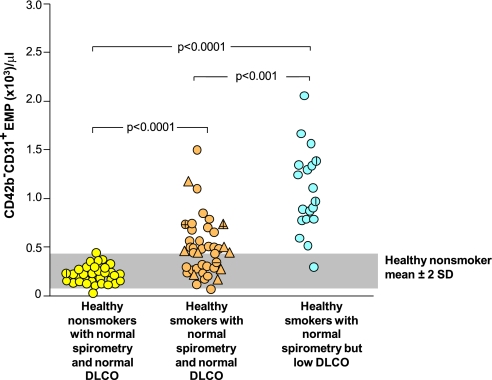
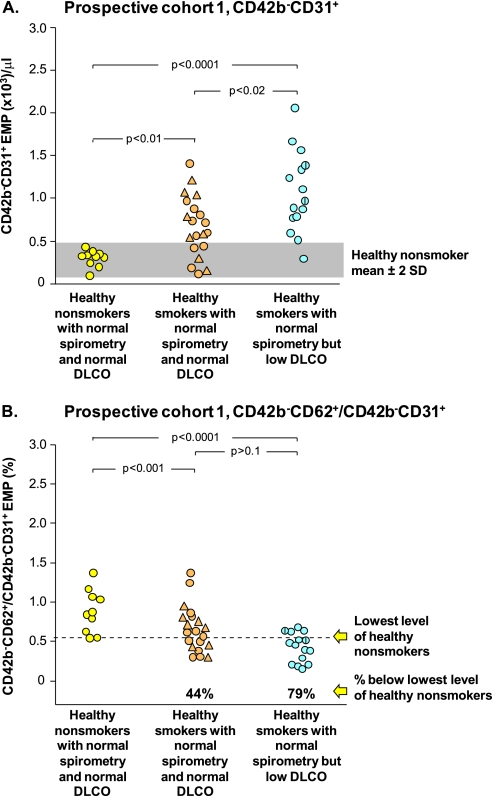
Methods: Lung health was assessed by pulmonary function tests (PFTs: spirometry, total lung capacity, Dl(co)) and chest X-ray; smoking status was assessed by urine nicotine and cotinine. EMP levels (CD42b(-)CD31(+) microparticles) were quantified as activated or apoptotic. The initial cohort (n = 92) included healthy nonsmokers (normal PFTs), healthy smokers (normal PFTs), and smokers with early evidence of lung destruction (normal spirometry, low Dl(co)). Two prospective cohorts were then tested: a group similar to the initial cohort and an HIV1(+) cohort.
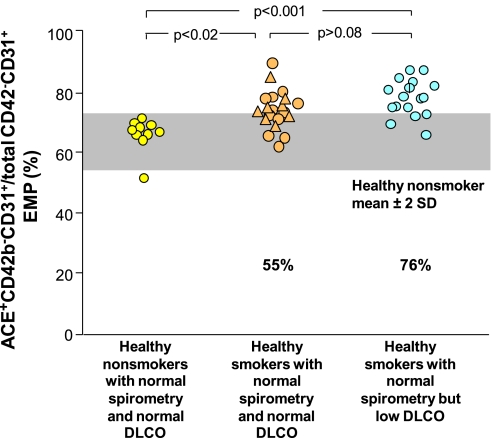
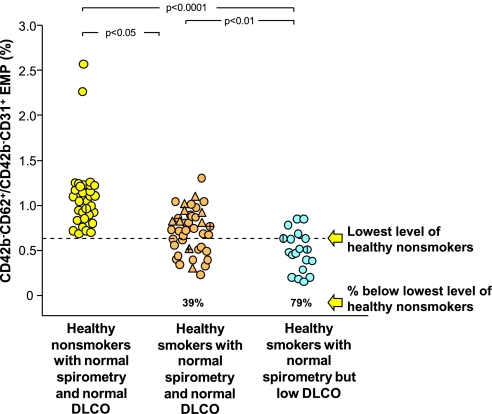
Measurements and main results: Healthy smokers had mildly increased levels of EMPs. Strikingly, 95% of smokers with normal spirometry, low Dl(co) had increased EMPs, with reduced CD62(+)/CD31(+) ratios (P < 10(-4)) and elevated CD42b(-)CD31(+) annexin V(+) EMPs (P < 10(-4)), suggesting derivation from endothelial apoptosis. Most elevated EMPs were angiotensin-converting enzyme positive, suggesting derivation from pulmonary capillaries. Both prospective cohorts confirmed the initial cohort data.
Conclusions: Plasma EMPs with apoptotic characteristics are elevated in smokers with normal spirometry but reduced Dl(co), consistent with the concept that emphysema is associated, in part, with capillary endothelium apoptosis, suggesting that the early development of emphysema might be monitored with plasma EMP levels.
Figures
Comment in
-
Endothelial chronic destructive pulmonary disease (E-CDPD): is endothelial apoptosis a subphenotype or prequel to COPD?Am J Respir Crit Care Med. 2011 Jul 15;184(2):153-5. doi: 10.1164/rccm.201104-0758ED. Am J Respir Crit Care Med. 2011. PMID: 21765029 No abstract available.
References
-
- Weibel ER. Morphological basis of alveolar-capillary gas exchange. Physiol Rev 1973;53:419–495 - PubMed
-
- Barnes PJ. Mediators of chronic obstructive pulmonary disease. Pharmacol Rev 2004;56:515–548 - PubMed
-
- Spurzem JR, Rennard SI. Pathogenesis of COPD. Semin Respir Crit Care Med 2005;26:142–153 - PubMed
-
- Abboud RT, Vimalanathan S. Pathogenesis of COPD. Part I. The role of protease-antiprotease imbalance in emphysema. Int J Tuberc Lung Dis 2008;12:361–367 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
