

Steroids and bronchodilators for acute bronchiolitis in the first two years of life: systematic review and meta-analysis
- PMID: 21471175
- PMCID: PMC3071611
- DOI: 10.1136/bmj.d1714
Steroids and bronchodilators for acute bronchiolitis in the first two years of life: systematic review and meta-analysis
Abstract
Objective: To evaluate and compare the efficacy and safety of bronchodilators and steroids, alone or combined, for the acute management of bronchiolitis in children aged less than 2 years.
Design: Systematic review and meta-analysis.
Data sources: Medline, Embase, Central, Scopus, PubMed, LILACS, IranMedEx, conference proceedings, and trial registers. Inclusion criteria Randomised controlled trials of children aged 24 months or less with a first episode of bronchiolitis with wheezing comparing any bronchodilator or steroid, alone or combined, with placebo or another intervention (other bronchodilator, other steroid, standard care).
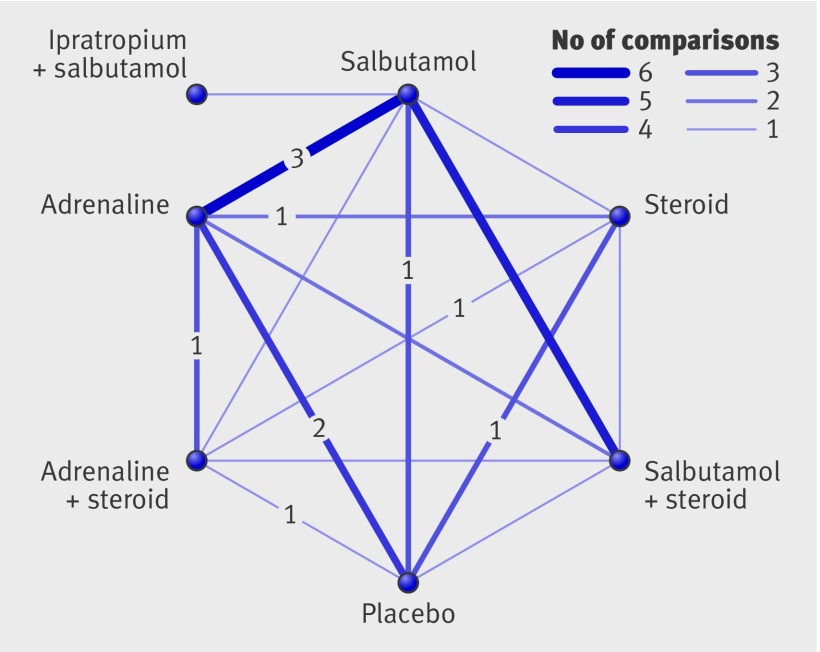
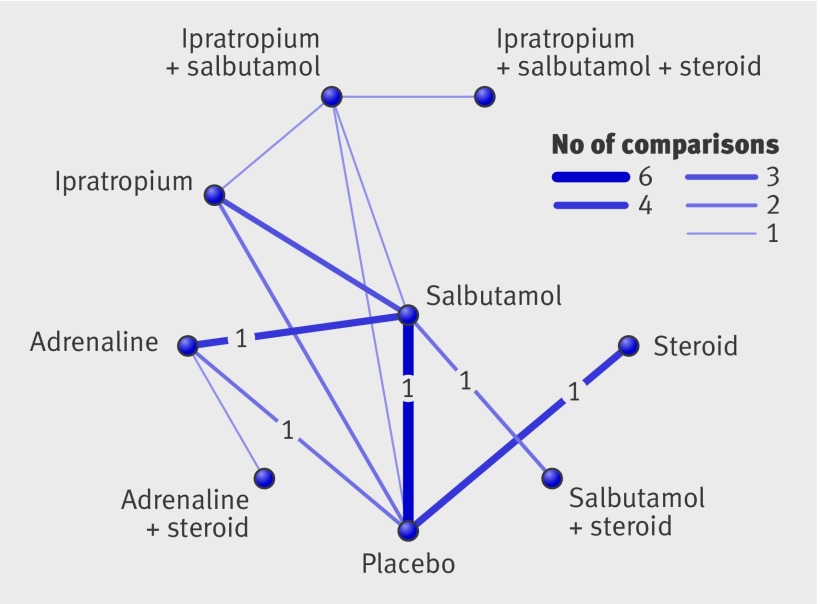
Review methods: Two reviewers assessed studies for inclusion and risk of bias and extracted data. Primary outcomes were selected by clinicians a priori based on clinical relevance: rate of admission for outpatients (day 1 and up to day 7) and length of stay for inpatients. Direct meta-analyses were carried out using random effects models. A mixed treatment comparison using a Bayesian network model was used to compare all interventions simultaneously.
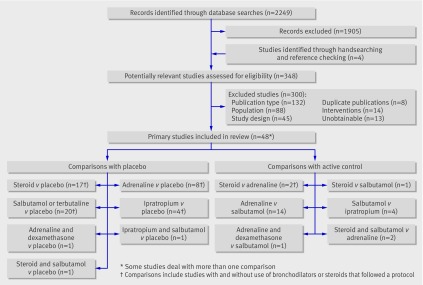
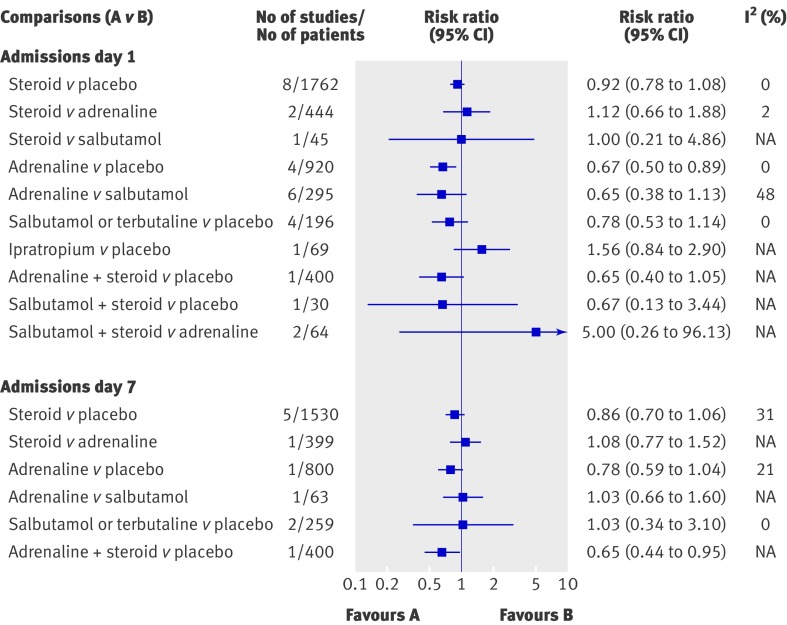
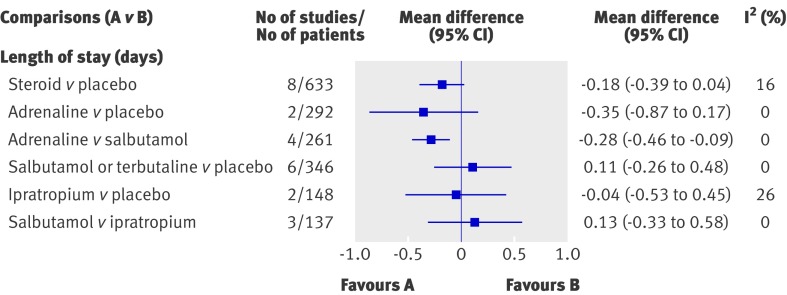
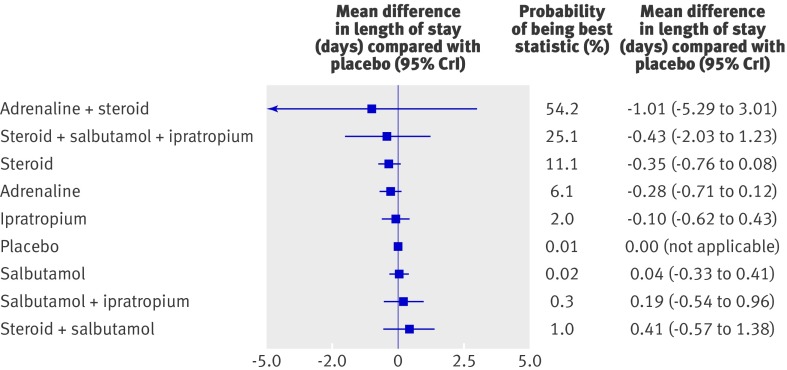
Results: 48 trials (4897 patients, 13 comparisons) were included. Risk of bias was low in 17% (n = 8), unclear in 52% (n = 25), and high in 31% (n = 15). Only adrenaline (epinephrine) reduced admissions on day 1 (compared with placebo: pooled risk ratio 0.67, 95% confidence interval 0.50 to 0.89; number needed to treat 15, 95% confidence interval 10 to 45 for a baseline risk of 20%; 920 patients). Unadjusted results from a single large trial with low risk of bias showed that combined dexamethasone and adrenaline reduced admissions on day 7 (risk ratio 0.65, 0.44 to 0.95; number needed to treat 11, 7 to 76 for a baseline risk of 26%; 400 patients). A mixed treatment comparison supported adrenaline alone or combined with steroids as the preferred treatments for outpatients (probability of being the best treatment based on admissions at day 1 were 45% and 39%, respectively). The incidence of reported harms did not differ. None of the interventions examined showed clear efficacy for length of stay among inpatients.
Conclusions: Evidence shows the effectiveness and superiority of adrenaline for outcomes of most clinical relevance among outpatients with acute bronchiolitis, and evidence from a single precise trial for combined adrenaline and dexamethasone.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures

Comment in
-
Management of acute bronchiolitis.BMJ. 2011 Apr 6;342:d1658. doi: 10.1136/bmj.d1658. BMJ. 2011. PMID: 21471173 No abstract available.
-
Flawed meta-analysis creates doubt when answers are known.BMJ. 2011 May 31;342:d3348. doi: 10.1136/bmj.d3348. BMJ. 2011. PMID: 21628368 No abstract available.
-
Epinephrine for acute bronchiolitis, but not steroids alone, reduces hospital admissions.Evid Based Med. 2012 Feb;17(1):12-3. doi: 10.1136/ebm.2011.100055. Epub 2011 Jun 24. Evid Based Med. 2012. PMID: 21705402 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical