

Association of Mycoplasma hominis infection with prostate cancer
- PMID: 21471611
- PMCID: PMC3248169
- DOI: 10.18632/oncotarget.256
Association of Mycoplasma hominis infection with prostate cancer
Abstract
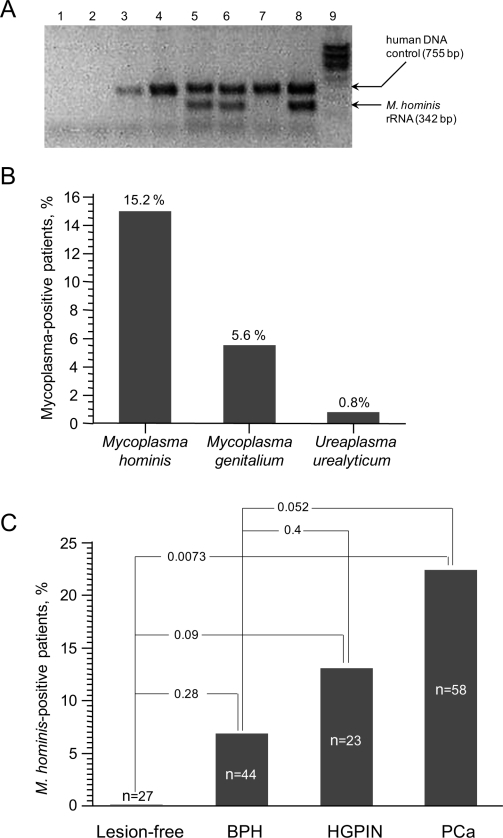
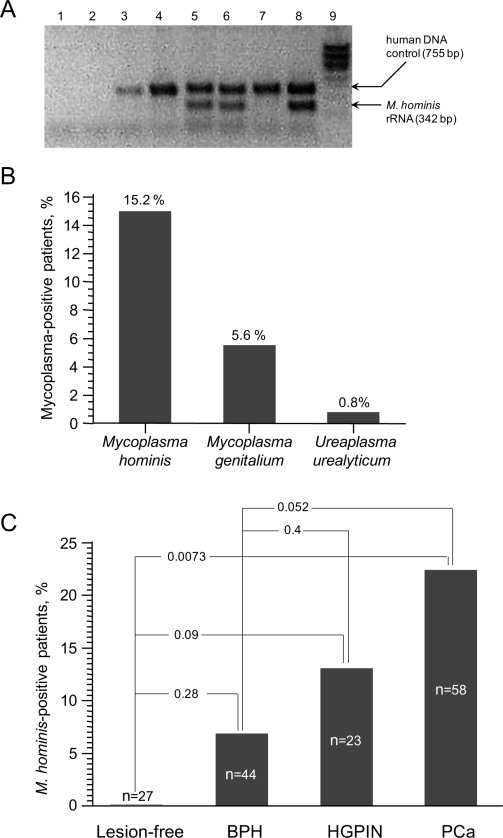
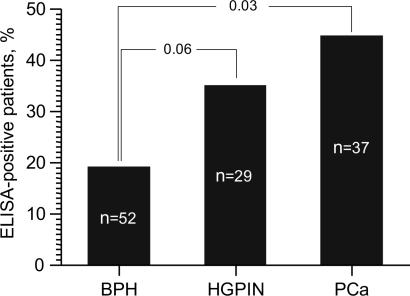
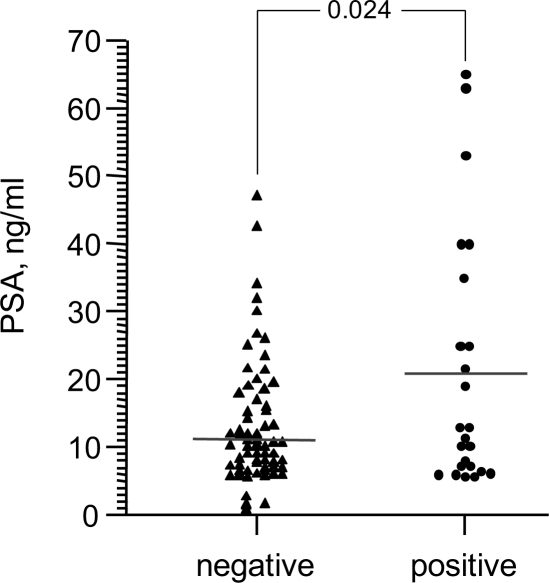
The origin of chronic inflammation preceding the development of prostate cancer (PCa) remains unknown. We investigated possible involvement of mycoplasma infection in PCa by screening prostate biopsies from two groups of Russian men undergoing PCa diagnosis. M. hominis was detected by standard PCR in 15% of the 125 patients in the first group and by quantitative real-time PCR in 37.4% of the 123 men in the second group. In both groups, stratification of patients according to diagnosis showed that M. hominis was present at three times higher frequency in patients with PCa than in those with benign prostatic hyperplasia. No M. hominis was detected in the prostates of 27 men without detectable prostate disease. In addition, PCa-positive men had higher titers of antibodies against M. hominis and average PSA levels were higher in M. hominis-positive men. These data, together with previous observations linking mycoplasma infection with cell transformation, genomic instability and resistance to apoptosis, suggest that M. hominis infection may be involved in PCa development and may, therefore, be a potential PCa marker and/or target for improved prevention and treatment of this disease.
Figures
Comment in
-
Mycoplasma and cancer: in search of the link.Oncotarget. 2011 Apr;2(4):271-3. doi: 10.18632/oncotarget.264. Oncotarget. 2011. PMID: 21508438 Free PMC article. No abstract available.
-
The "infectious" nature of human prostate cancer: a cautionary note.Oncotarget. 2011 Apr;2(4):281-3. doi: 10.18632/oncotarget.267. Oncotarget. 2011. PMID: 21521904 Free PMC article. No abstract available.
-
Mycoplasmas and human prostate cancer: an exciting but cautionary note.Oncotarget. 2011 May;2(5):352-5. doi: 10.18632/oncotarget.282. Oncotarget. 2011. PMID: 21789784 Free PMC article. No abstract available.
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun M. Cancer Statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Karin M, Lawrence T, Nizet V. Innate immunity gone awry: linking microbial infections to chronic inflammation and cancer. Cell. 2006;124:823–35. - PubMed
-
- Sutcliffe S, Platz EA. Inflammation and prostate cancer: a focus on infections. Curr Urol Rep. 2008;9:243–9. - PubMed
-
- Wagenlehner FM, Elkahwaji JE, Algaba F, Bjerklund-Johansen T, Naber KG, Hartung R, Weidner W. The role of inflammation and infection in the pathogenesis of prostate carcinoma. BJU Int. 2007;100:733–7. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
