

Hospital racial composition: a neglected factor in cardiac arrest survival disparities
- PMID: 21473969
- PMCID: PMC3073775
- DOI: 10.1016/j.ahj.2011.01.011
Hospital racial composition: a neglected factor in cardiac arrest survival disparities
Abstract
Background: Racial disparities in survival after out-of-hospital cardiac arrest have been reported, but their causes remain uncertain. We sought to determine if hospital racial composition accounted for survival differences for patients hospitalized after cardiac arrest.
Methods: We evaluated hospitalizations of white and black Medicare beneficiaries (2000-2007) admitted from the emergency department to the intensive care unit with a diagnosis of cardiac arrest or ventricular fibrillation. We examined unadjusted survival rates and developed a multivariable logistic regression model that included patient and hospital factors.
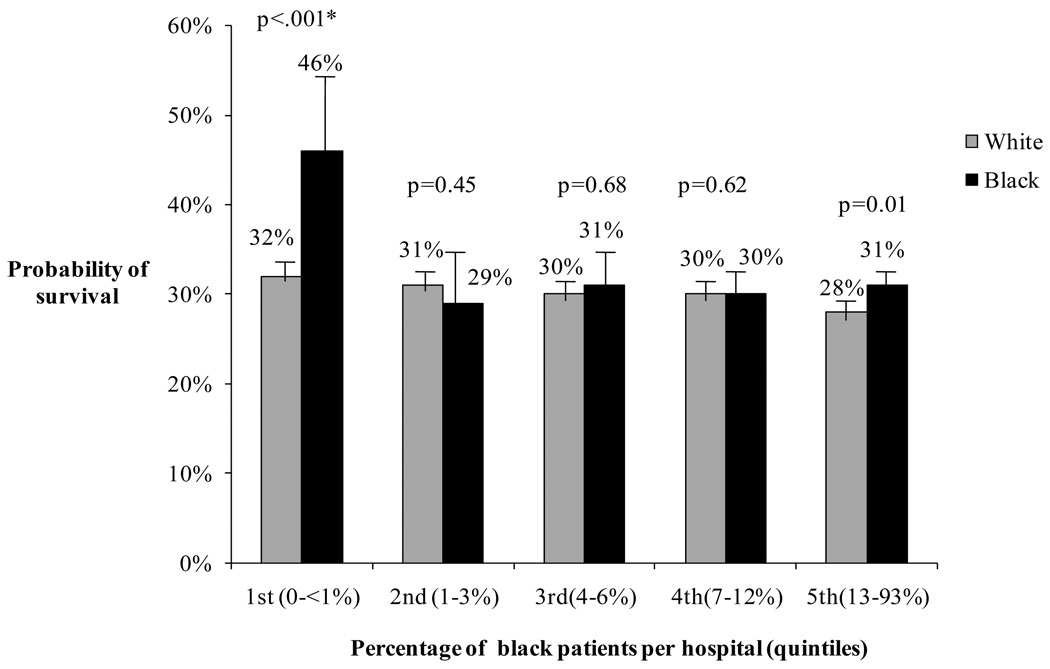
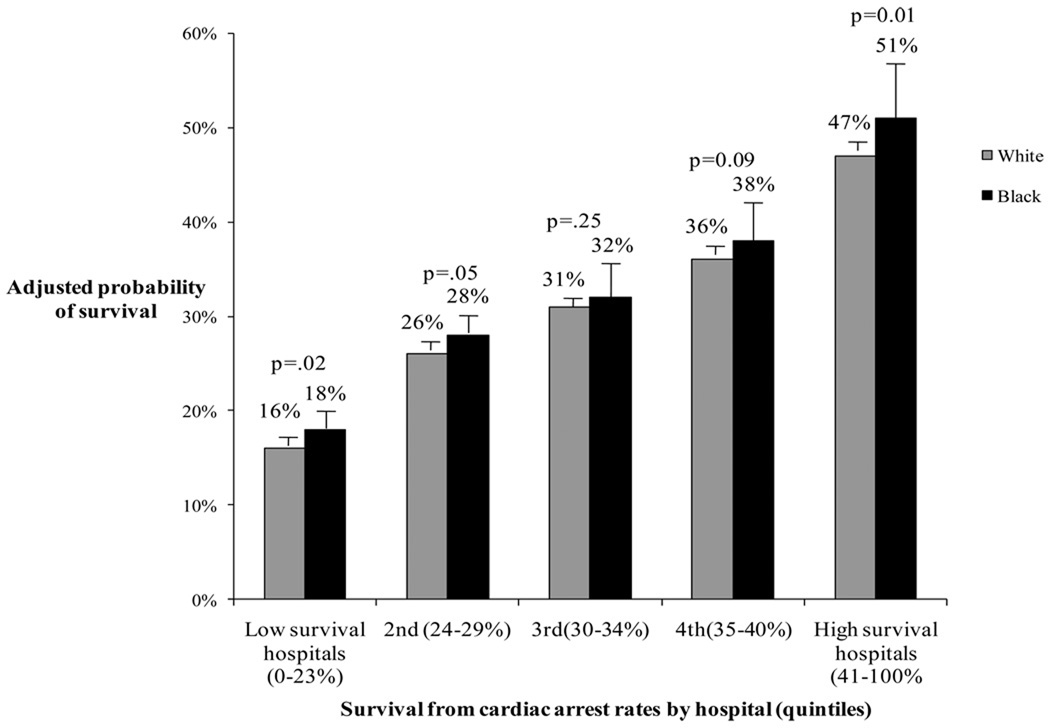
Results: We analyzed 68,115 cardiac arrest admissions. Unadjusted survival to hospital discharge was worse for blacks (n = 7,942) compared with whites (n = 60,173) (30% vs 33%, P < .001). In multivariate analyses accounting for patient and hospital factors, adjusted probability of survival was worse for black patients at hospitals with higher proportions of black patients (31%, 95% CI 29%-32%) compared with predominately white hospitals (46%, 95% CI 36%-57%; P = .003). Similarly, whites had worse risk-adjusted survival at hospitals with higher proportions of black patients (28%, 95% CI 27%-30%) compared with predominately white hospitals (32%, 95% CI 31%-33%, P = .006). Blacks were more likely to be admitted to hospitals with low survival rates (23% vs 15%, P < .001).
Conclusion: Hospitals with large black patient populations had worse cardiac arrest outcomes than predominantly white hospitals, and blacks were more likely to be admitted to these high-mortality hospitals. Understanding these differences in survival outcomes may uncover the causes for these disparities and lead to improved survival for all cardiac arrest victims.
Copyright © 2011 Mosby, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Becker LB, Han BH, Meyer PM, et al. Racial differences in the incidence of cardiac arrest and subsequent survival. The CPR Chicago Project. N Engl J Med. 1993;329:600–606. - PubMed
-
- Iwashyna TJ, Christakis NA, Becker LB. Neighborhoods matter: a population-based study of provision of cardiopulmonary resuscitation. Ann Emerg Med. 1999;34:459–468. - PubMed
-
- Galea S, Blaney S, Nandi A, et al. Explaining racial disparities in incidence of and survival from out-of-hospital cardiac arrest. Am J Epidemiol. 2007;166:534–543. - PubMed
-
- Brookoff D, Kellermann AL, Hackman BB, Somes G, Dobyns P. Do blacks get bystander cardiopulmonary resuscitation as often as whites? Ann Emerg Med. 1994;24:1147–1150. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
