

Projected impact of polypill use among US adults: Medication use, cardiovascular risk reduction, and side effects
- PMID: 21473971
- PMCID: PMC3093765
- DOI: 10.1016/j.ahj.2010.12.019
Projected impact of polypill use among US adults: Medication use, cardiovascular risk reduction, and side effects
Abstract
Background: Polypills, which include multiple medications for reducing cardiovascular disease (CVD) risk in a single pill, have been proposed for population-wide use. The number of US adults eligible for polypills and potential benefits are unknown.
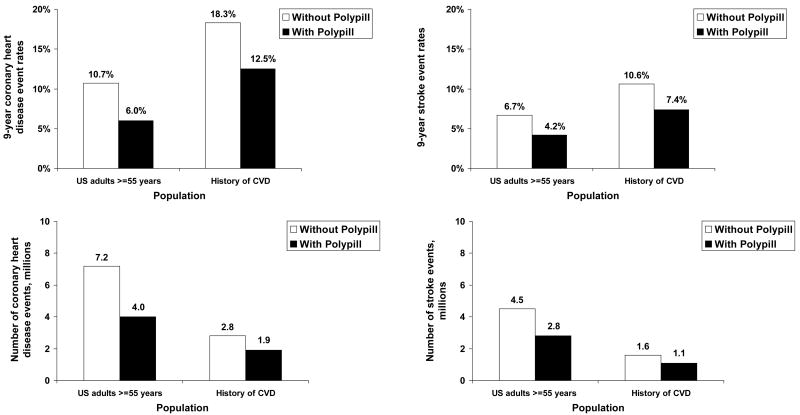
Methods: The National Health and Nutrition Examination Survey 2003-2004 and 2007-2008 were analyzed to estimate treatment rates for medications proposed for inclusion in polypills (aspirin, statin, an angiotensin-converting enzyme [ACE] inhibitor, and a thiazide-type diuretic for those without and a β-blocker for those with a history of myocardial infarction) among US adults. The number of coronary heart disease (CHD) and stroke events potentially prevented through polypill use was projected by published meta-analyses and 3 large population-based cohort studies. Two polypill eligibility criteria were analyzed: (1) US adults ≥55 years and (2) US adults with a history of CVD.
Results: There are 67.6 million US adults ≥55 years and 15.4 million US adults with a history of CVD and, thus, eligible for polypills using the 2 outlined criteria. In 2007 to 2008, 37.3% of US adults ≥55 years and 57.0% of those with a history of CVD were taking statins. Use of other polypill medications was also low. Polypill use by US adults aged ≥55 years is projected to potentially prevent 3.2 million CHD events and 1.7 million strokes over 10 years. Among those with a history of CVD, the potential to prevent of 0.9 million CHD events and 0.5 million strokes is projected.
Conclusions: Polypills have the potential to lower CVD incidence substantially among US adults.
Copyright © 2011 Mosby, Inc. All rights reserved.
Conflict of interest statement
Disclosures: The authors have no potential conflicts of interest to report.
Figures
References
-
- World Health Organization. WHO-Wellcome Trust meeting report 1-3. Geneva: 2002. Secondary prevention of non-communicable disease in low and middle income countries through community-based and health service interventions.
-
- Watts G. What happened to the polypill? BMJ. 2008;337:a1822. - PubMed
-
- Fuster V, Sanz G. A polypill for secondary prevention: time to move from intellectual debate to action. Nat Clin Pract Cardiovasc Med. 2007;4(4):173. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
