

Lifetime risks for cardiovascular disease mortality by cardiorespiratory fitness levels measured at ages 45, 55, and 65 years in men. The Cooper Center Longitudinal Study
- PMID: 21474041
- PMCID: PMC3608397
- DOI: 10.1016/j.jacc.2010.10.056
Lifetime risks for cardiovascular disease mortality by cardiorespiratory fitness levels measured at ages 45, 55, and 65 years in men. The Cooper Center Longitudinal Study
Abstract
Objectives: The purpose of this study was to determine the association between fitness and lifetime risk for cardiovascular disease (CVD).
Background: Higher levels of traditional risk factors are associated with marked differences in lifetime risks for CVD. However, data are sparse regarding the association between fitness and the lifetime risk for CVD.
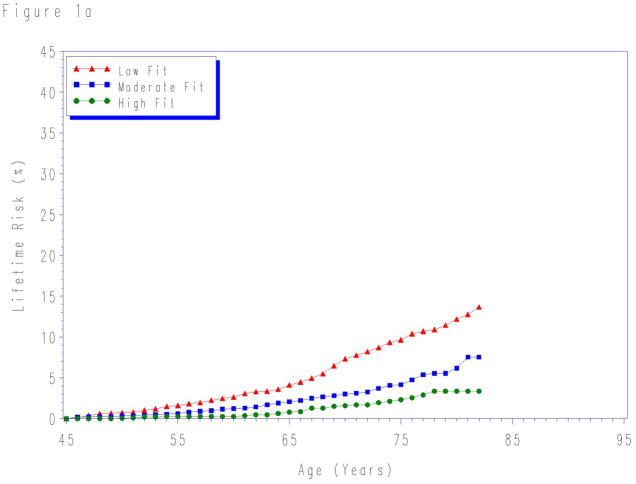
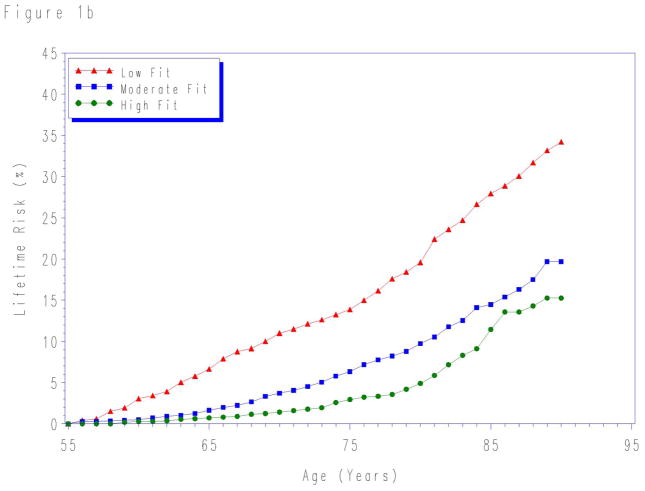
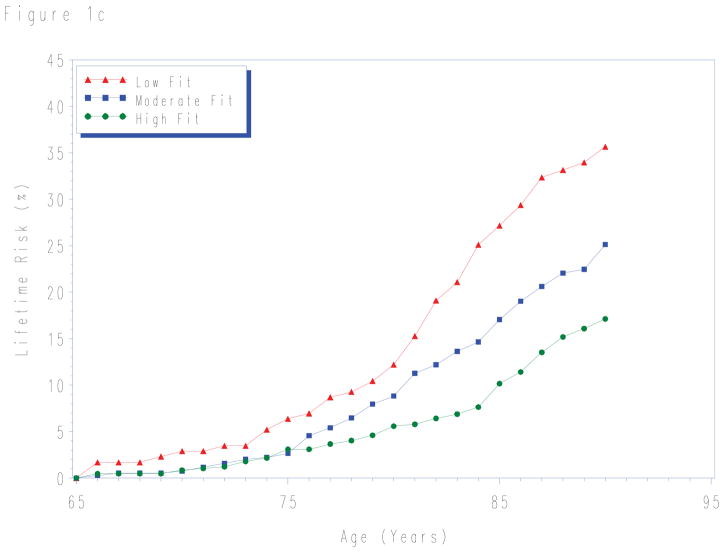
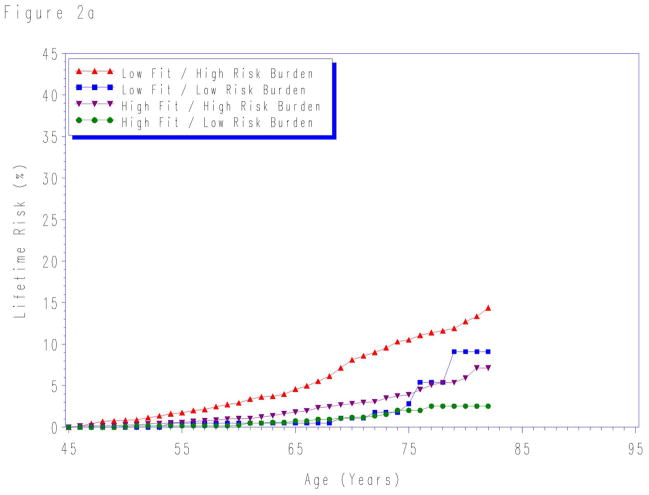
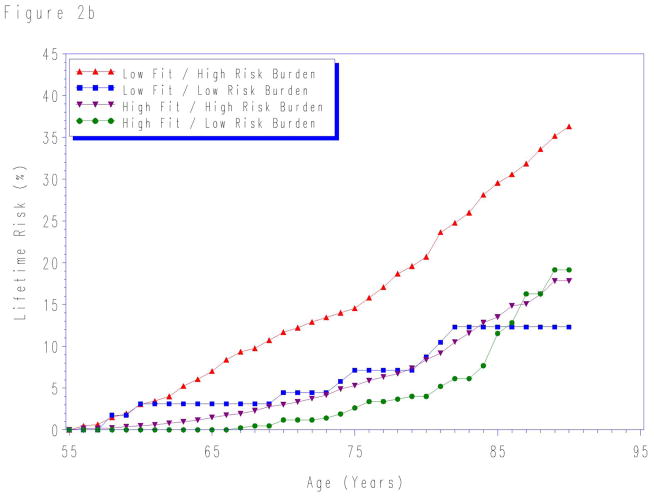
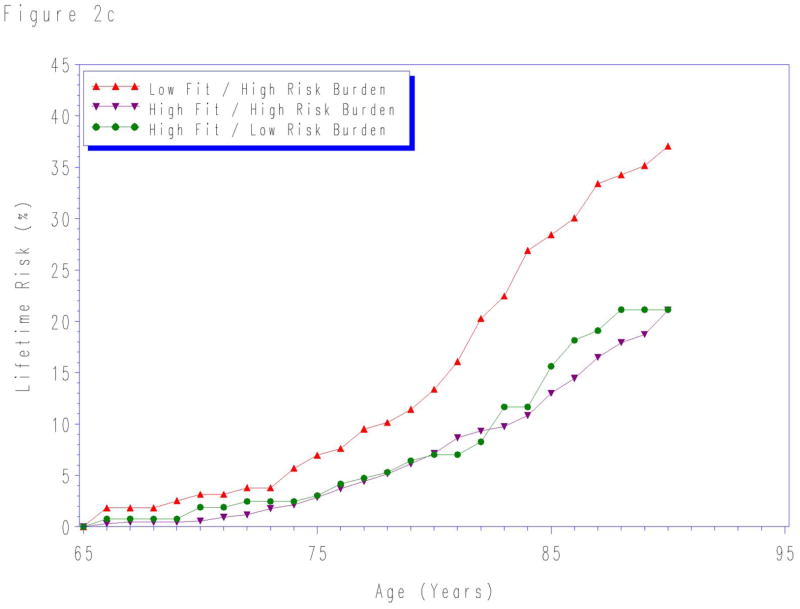
Methods: We followed up 11,049 men who underwent clinical examination at the Cooper Institute in Dallas, Texas, before 1990 until the occurrence of CVD death, non-CVD death, or attainment of age 90 years (281,469 person-years of follow-up, median follow-up 25.3 years, 1,106 CVD deaths). Fitness was measured by the Balke protocol and categorized according to treadmill time into low, moderate, and high fitness, with further stratification by CVD risk factor burden. Lifetime risk for CVD death determined by the National Death Index was estimated for fitness levels measured at ages 45, 55, and 65 years, with non-CVD death as the competing event.
Results: Differences in fitness levels (low fitness vs. high fitness) were associated with marked differences in the lifetime risks for CVD death at each index age: age 45 years, 13.7% versus 3.4%; age 55 years, 34.2% versus 15.3%; and age 65 years, 35.6% versus 17.1%. These associations were strongest among persons with CVD risk factors.
Conclusions: A single measurement of low fitness in mid-life was associated with higher lifetime risk for CVD death, particularly among persons with a high burden of CVD risk factors.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Is cardiorespiratory fitness a unique cardiovascular disease risk factor?J Am Coll Cardiol. 2011 Sep 13;58(12):1284; author reply 1284-5. doi: 10.1016/j.jacc.2011.05.045. J Am Coll Cardiol. 2011. PMID: 21903066 No abstract available.
References
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–6. - PubMed
-
- Schoenborn CA, Adams PF, Barnes PM, Vickerie JL, Schiller JS. Health behaviors of adults: United States, 1999–2001. Vital Health Stat. 2004;10:1–79. - PubMed
-
- Blair SN, Kohl HW, Barlow CE, Paffenbarger RS, Gibbons LW, Macera CA. Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA. 1995;273:1093–8. - PubMed
-
- Blair SN, Kohl HW, 3rd, Paffenbarger RS, Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. 1989;262:2395–401. - PubMed
-
- Ekelund LG, Haskell WL, Johnson JL, Whaley FS, Criqui MH, Sheps DS. Physical fitness as a predictor of cardiovascular mortality in asymptomatic North American men. The Lipid Research Clinics Mortality Follow-up Study. N Engl J Med. 1988;319:1379–84. - PubMed
