

Review articles: postoperative delirium: acute change with long-term implications
- PMID: 21474660
- PMCID: PMC3090222
- DOI: 10.1213/ANE.0b013e3182147f6d
Review articles: postoperative delirium: acute change with long-term implications
Abstract
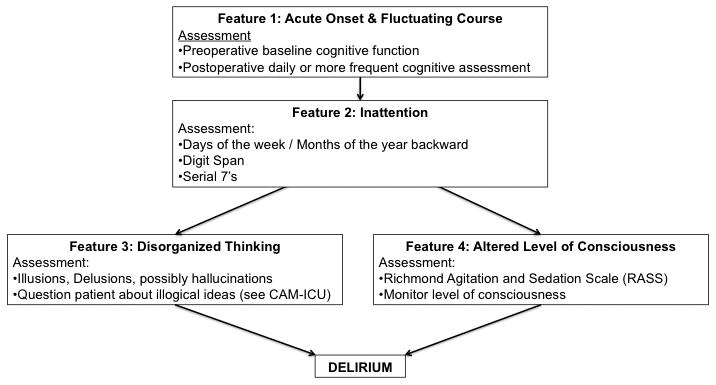
Delirium is an acute change in cognition and attention, which may include alterations in consciousness and disorganized thinking. Although delirium may affect any age group, it is most common in older patients, especially those with preexisting cognitive impairment. Patients with delirium after surgery recover more slowly than those without delirium and, as a result, have increased length of stay and hospital costs. The measured incidence of postoperative delirium varies with the type of surgery, the urgency of surgery, and the type and sensitivity of the delirium assessment. Although generally considered a short-term condition, delirium can persist for months and is associated with poor cognitive and functional outcomes beyond the immediate postoperative period. In this article, we provide a guide to assess delirium risk preoperatively and to prevent, diagnose, and treat this common and morbid condition. Care improvements such as identifying delirium risk preoperatively; training surgeons, anesthesiologists, and nurses to screen for delirium; implementing delirium prevention programs; and developing standardized delirium treatment protocols may reduce the risk of delirium and its associated morbidity.
© 2011 International Anesthesia Research Society
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Rudolph JL, Jones RN, Rasmussen LS, Silverstein JH, Inouye SK, Marcantonio ER. Independent vascular and cognitive risk factors for postoperative delirium. Am J Med. 2007;120:807–13. - PubMed
-
- Marcantonio ER, Goldman L, Mangione CM, Ludwig LE, Muraca B, Haslauer CM, Donaldson MC, Whittemore AD, Sugarbaker DJ, Poss R, Haas S, Cook EF, Orav EJ, Lee TH. A clinical prediction rule for delirium after elective noncardiac surgery. JAMA. 1994;271:134–9. - PubMed
-
- Norkiene I, Ringaitiene D, Misiuriene I, Samalavicius R, Bubulis R, Baublys A, Uzdavinys G. Incidence and precipitating factors of delirium after coronary artery bypass grafting. Scand Cardiovasc J. 2007;41:180–5. - PubMed
-
- Marcantonio ER, Flacker JM, Michaels M, Resnick NM. Delirium is independently associated with poor functional recovery after hip fracture. J Am Geriatr Soc. 2000;48:618–24. - PubMed
-
- Robinson TN, Raeburn CD, Tran ZV, Angles EM, Brenner LA, Moss M. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg. 2009;249:173–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
