

Pituitary incidentaloma: an endocrine society clinical practice guideline
- PMID: 21474686
- PMCID: PMC5393422
- DOI: 10.1210/jc.2010-1048
Pituitary incidentaloma: an endocrine society clinical practice guideline
Abstract
Objective: The aim was to formulate practice guidelines for endocrine evaluation and treatment of pituitary incidentalomas.
Consensus process: Consensus was guided by systematic reviews of evidence and discussions through a series of conference calls and e-mails and one in-person meeting.
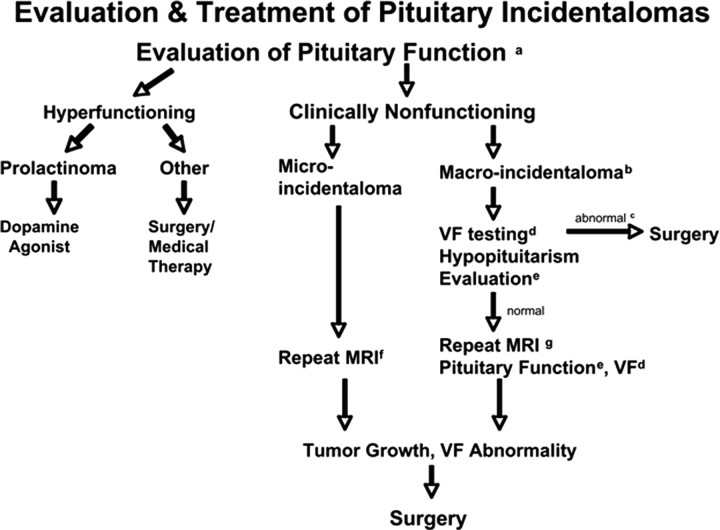
Conclusions: We recommend that patients with a pituitary incidentaloma undergo a complete history and physical examination, laboratory evaluations screening for hormone hypersecretion and for hypopituitarism, and a visual field examination if the lesion abuts the optic nerves or chiasm. We recommend that patients with incidentalomas not meeting criteria for surgical removal be followed with clinical assessments, neuroimaging (magnetic resonance imaging at 6 months for macroincidentalomas, 1 yr for a microincidentaloma, and thereafter progressively less frequently if unchanged in size), visual field examinations for incidentalomas that abut or compress the optic nerve and chiasm (6 months and yearly), and endocrine testing for macroincidentalomas (6 months and yearly) after the initial evaluations. We recommend that patients with a pituitary incidentaloma be referred for surgery if they have a visual field deficit; signs of compression by the tumor leading to other visual abnormalities, such as ophthalmoplegia, or neurological compromise due to compression by the lesion; a lesion abutting the optic nerves or chiasm; pituitary apoplexy with visual disturbance; or if the incidentaloma is a hypersecreting tumor other than a prolactinoma.
Figures
Comment in
-
Whither pituitary incidentaloma?J Clin Endocrinol Metab. 2011 Apr;96(4):939-41. doi: 10.1210/jc.2011-0415. J Clin Endocrinol Metab. 2011. PMID: 21474690 No abstract available.
References
-
- Atkins D , Best D , Briss PA , Eccles M , Falck-Ytter Y , Flottorp S , Guyatt GH , Harbour RT , Haugh MC , Henry D , Hill S , Jaeschke R , Leng G , Liberati A , Magrini N , Mason J , Middleton P , Mrukowicz J , O'Connell D , Oxman AD , Phillips B , Schünemann HJ , Edejer TT , Varonen H , Vist GE , Williams JW , Zaza S. 2004. Grading quality of evidence and strength of recommendations. BMJ 328:1490. - PMC - PubMed
-
- Swiglo BA , Murad MH , Schünemann HJ , Kunz R , Vigersky RA , Guyatt GH , Montori VM. 2008. A case for clarity, consistency, and helpfulness: state-of-the-art clinical practice guidelines in endocrinology using the grading of recommendations, assessment, development, and evaluation system. J Clin Endocrinol Metab 93:666–673 - PubMed
-
- Fernandez-Balsells M MM , Barwise A , Gallegos-Orozco J , Paul A , Lane M , Carpio I , Perestelo-Perez LI , Ponce de Leon Lovaton P , Erwin P , Carey J , Montori VM. 2010. The natural history of pituitary incidentalomas: a systematic review and meta-analysis. J Clin Endocrinol Metab (In press) - PubMed
-
- Feldkamp J , Santen R , Harms E , Aulich A , Mödder U , Scherbaum WA. 1999. Incidentally discovered pituitary lesions: high frequency of macroadenomas and hormone-secreting adenomas—results of a prospective study. Clin Endocrinol (Oxf) 51:109–113 - PubMed
-
- Arita K , Tominaga A , Sugiyama K , Eguchi K , Iida K , Sumida M , Migita K , Kurisu K. 2006. Natural course of incidentally found nonfunctioning pituitary adenoma, with special reference to pituitary apoplexy during follow-up examination. J Neurosurg 104:884–891 - PubMed
