

Intraoperative imaging guidance for sentinel node biopsy in melanoma using a mobile gamma camera
- PMID: 21475019
- PMCID: PMC4775232
- DOI: 10.1097/SLA.0b013e3181f9b709
Intraoperative imaging guidance for sentinel node biopsy in melanoma using a mobile gamma camera
Abstract
Objective: To evaluate the sensitivity and clinical utility of intraoperative mobile gamma camera (MGC) imaging in sentinel lymph node biopsy (SLNB) in melanoma.
Background: The false-negative rate for SLNB for melanoma is approximately 17%, for which failure to identify the sentinel lymph node (SLN) is a major cause. Intraoperative imaging may aid in detection of SLN near the primary site, in ambiguous locations, and after excision of each SLN. The present pilot study reports outcomes with a prototype MGC designed for rapid intraoperative image acquisition. We hypothesized that intraoperative use of the MGC would be feasible and that sensitivity would be at least 90%.
Methods: From April to September 2008, 20 patients underwent Tc99 sulfur colloid lymphoscintigraphy, and SLNB was performed with use of a conventional fixed gamma camera (FGC), and gamma probe followed by intraoperative MGC imaging. Sensitivity was calculated for each detection method. Intraoperative logistical challenges were scored. Cases in which MGC provided clinical benefit were recorded.
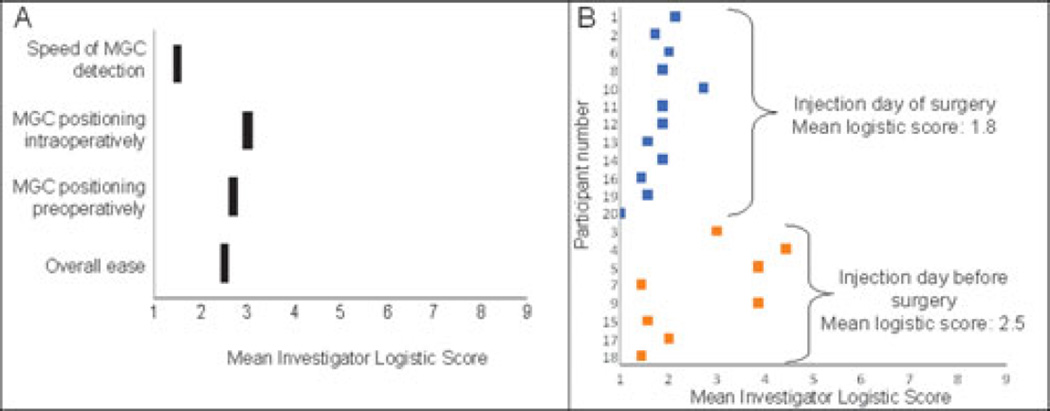
Results: Sensitivity for detecting SLN basins was 97% for the FGC and 90% for the MGC. A total of 46 SLN were identified: 32 (70%) were identified as distinct hot spots by preoperative FGC imaging, 31 (67%) by preoperative MGC imaging, and 43 (93%) by MGC imaging pre- or intraoperatively. The gamma probe identified 44 (96%) independent of MGC imaging. The MGC provided defined clinical benefit as an addition to standard practice in 5 (25%) of 20 patients. Mean score for MGC logistic feasibility was 2 on a scale of 1-9 (1 = best).
Conclusions: Intraoperative MGC imaging provides additional information when standard techniques fail or are ambiguous. Sensitivity is 90% and can be increased. This pilot study has identified ways to improve the usefulness of an MGC for intraoperative imaging, which holds promise for reducing false negatives of SLNB for melanoma.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



References
-
- Testori A, De Salvo GL, Montesco MC, et al. Clinical considerations on sentinel node biopsy in melanoma from an Italian multicentric study on 1,313 patients (SOLISM-IMI) Ann Surg Oncol. 2009;16(7):2018–2027. - PubMed
-
- Karim RZ, Scolyer RA, Li W, et al. False negative sentinel lymph node biopsies in melanoma may result from deficiencies in nuclear medicine, surgery, or pathology. Ann Surg. 2008;247:1003–1010. - PubMed
-
- Caraco C, Marone U, Celentano E, et al. Impact of false-negative sentinel lymph node biopsy on survival in patients with cutaneous melanoma. Ann Surg Oncol. 2007;14:2662–2667. - PubMed
-
- Clary BM, Mann B, Brady MS, et al. Early recurrence after lymphatic mapping and sentinel node biopsy in patients with primary extremity melanoma: a comparison with elective lymph node dissection. Ann Surg Oncol. 2001;8:328–337. - PubMed
-
- Mathelin C, Salvador S, Huss D, et al. Precise localization of sentinel lymph nodes and estimation of their depth using a prototype intraoperative mini gamma-camera in patients with breast cancer. J Nucl Med. 2007;48:623–629. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
