

Prevalence of ocular motor cranial nerve palsy and associations following stroke
- PMID: 21475314
- PMCID: PMC3178159
- DOI: 10.1038/eye.2011.78
Prevalence of ocular motor cranial nerve palsy and associations following stroke
Abstract
Aim: Occurrence of ocular motor cranial nerve palsies (OMCNP), following stroke, has not been reported in relation to the type of OMCNP seen and in relation to brain area affected by stroke. The aim of this study was to identify all patients referred with suspected visual impairment to establish the presence and type of OMCNP.
Methods: Prospective, observation study with standardised referral and assessment forms across 20 sites. Visual assessment included visual acuity measurement, visual field assessment, ocular alignment, and movement and visual inattention assessment. Multicentre ethics approval and informed patient consent was obtained.
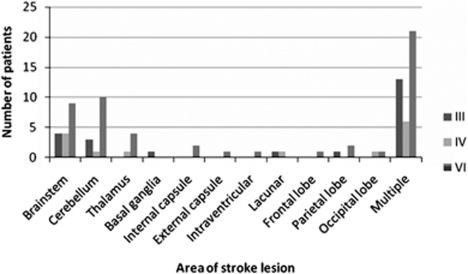
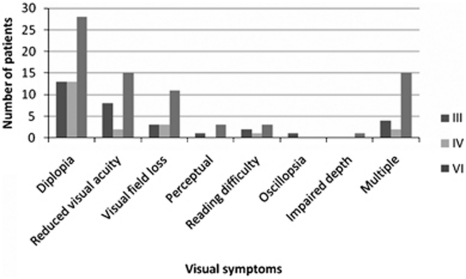
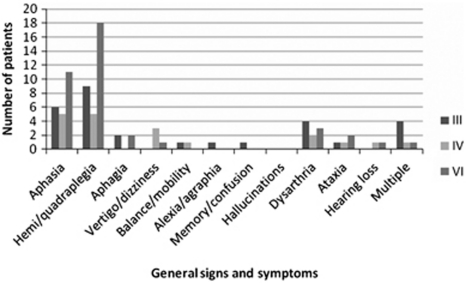
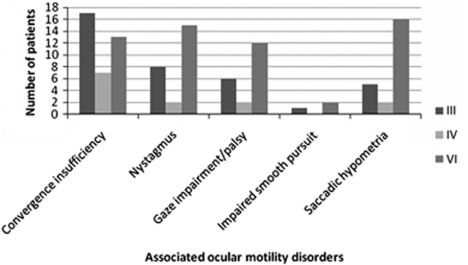
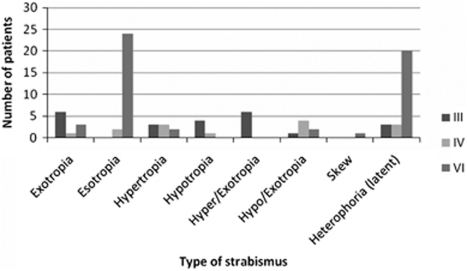
Results: In total, 915 patients were recruited with mean age of 69.18 years (SD 14.19). Altogether, 498 patients (54%) were diagnosed with ocular motility abnormalities. Of these, 89 patients (18%) had OMCNP. Unilateral third nerve palsy was present in 23 patients (26%), fourth nerve palsy in 14 patients (16%), and sixth nerve palsy in 52 patients (58%). Out of these, 44 patients had isolated OMCNP and 45 had OMCNP combined with other ocular motility abnormalities. Location of stroke was reported mainly in cerebellum, brain stem, thalamus, and internal and external capsules. Treatment was provided for each case including prisms, occlusion, typoscope, scanning exercises, and refraction.
Conclusions: OMCNP account for 18% of eye movement abnormalities in this stroke sub-population. Sixth CNP was most common, followed by third and fourth CNP. Half were isolated and half combined with other eye movement abnormality. Most were treated with prisms or occlusion. The reported brain area affected by stroke was typically the cerebellum, brain stem, and diencephalic structures.
Figures
References
-
- Rucker CW. Paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol. 1958;46:787–794. - PubMed
-
- Rush JA, Younge BR. Paralysis of cranial nerves III, IV and VI. Cause and prognosis in1000 cases. Arch Ophthalmol. 1981;99:76–79. - PubMed
-
- Rucker CW. The causes of paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol. 1966;61:1293–1298. - PubMed
-
- Richards BW, Jones FR, Younge BR. Causes and prognosis in 4278 cases of paralysis of the oculomotor, trochlear and abducens cranial nerves. Am J Ophthalmol. 1992;113:489–496. - PubMed
-
- Fowler MS, Wade DT, Richardson AJ, Stein JF. Squints and diplopia seen after brain damage. J Neurol. 1996;243:86–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
