

Assessment of scaphoid fracture healing
- PMID: 21475561
- PMCID: PMC3070004
- DOI: 10.1007/s12178-011-9072-0
Assessment of scaphoid fracture healing
Abstract
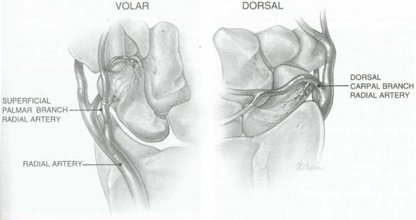
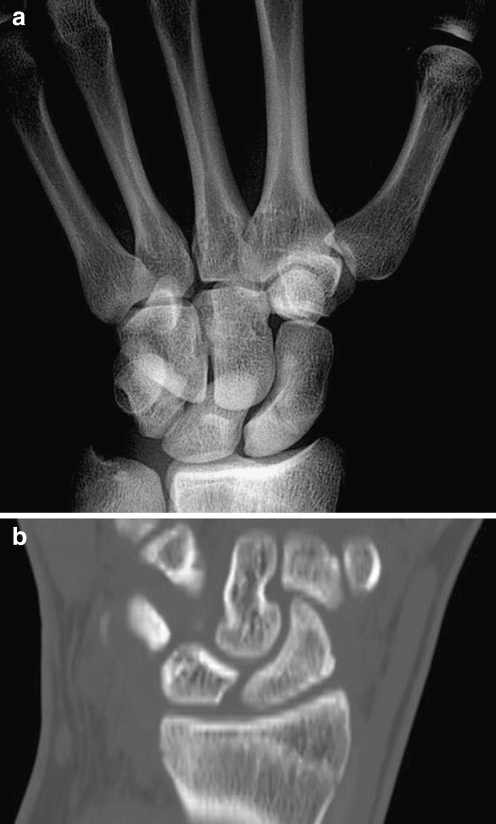
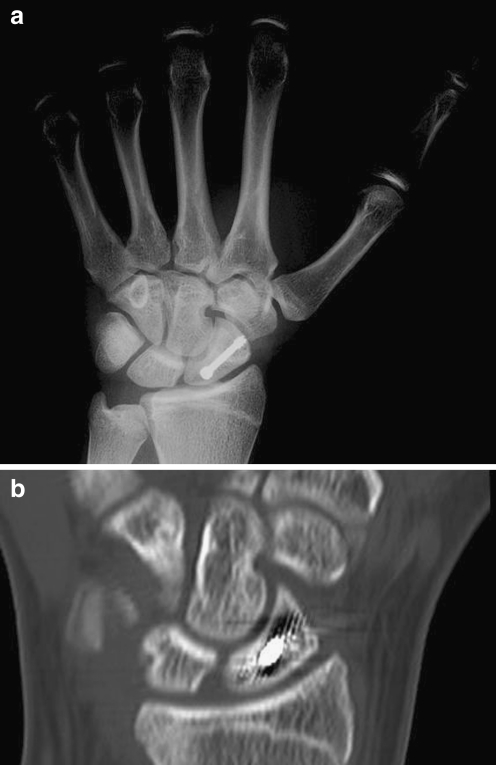
Scaphoid fractures are among the most common hand fractures in adults. The geometry of the scaphoid as it relates to its retrograde blood supply renders it particularly prone to avascular necrosis and other fracture complications. Though there has been long-standing debate over the optimal method of diagnosing scaphoid fractures, the best and most cost-effective methods combine clinical exam with other imaging modalities such as navicular view plain films, CT, and MRI for particularly questionable presentations. Once a scaphoid fracture is diagnosed, it should be followed by an orthopaedic surgeon and treated with cast immobilization or operative management in the case of displaced fractures. Fractures should be followed to monitor healing progress in order to ensure the eventual development of bridging bone across the fracture line, usually best appreciated on CT. Proper treatment of scaphoid fractures and assessment of fracture healing can minimize the occurrence of non-unions and associated arthritic changes.
Keywords: Healing; Imaging; Non-union; Scaphoid fracture.
Figures



References
-
- Gaebler C, McQueen MM. Carpus fractures and dislocations. In: Bucholz RW, Heckman JD, Court-Brown CM, Tornetta P, editors. Fractures in adults. 3. Philadelphia: Lippincott Williams and Wilkins; 2009. pp. 782–828.
-
- Ring D, Jupiter J, Herndon J. Acute fractures of the scaphoid. J Am Acad Orthop Surg. 2000;8:225–231. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
