

Femoroacetabular impingement: a review of diagnosis and management
- PMID: 21475562
- PMCID: PMC3070009
- DOI: 10.1007/s12178-011-9073-z
Femoroacetabular impingement: a review of diagnosis and management
Erratum in
-
Erratum to: Femoroacetabular impingement: a review of diagnosis and management.Curr Rev Musculoskelet Med. 2012 Dec;5(4):315. doi: 10.1007/s12178-012-9136-9. Curr Rev Musculoskelet Med. 2012. PMID: 22851012 Free PMC article. No abstract available.
Abstract
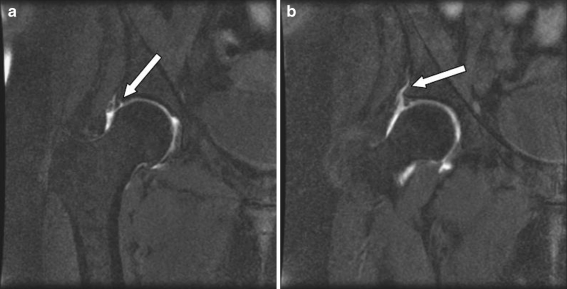
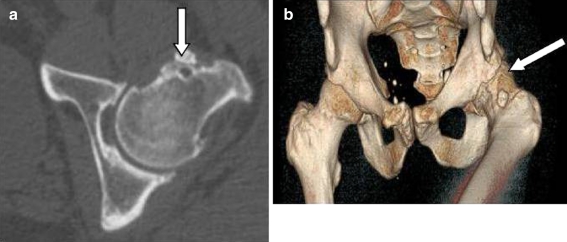
Hip pain in adults has traditionally been associated with osteoarthritis in the joint. However, many young patients with hip pain do get referred to orthopaedic surgeons without arthritis. Subtle bony and soft tissues abnormalities can present with hip pain in the active young adult. These abnormalities can lead to premature arthritis. With the improvements in clinical examination for hip impingement, radiological imaging using magnetic resonance arthrography (MRA) and or computed tomograms (CT) Scans, these lesions are being detected early. Though the cause of primary osteoarthritis is unknown, it is suggested that femoro-acetabular impingement (FAI) may be responsible for the progression of the disease in these patients. FAI is a pathological condition leading to abutment between the proximal femur and the acetabular rim. Two different mechanisms are described, although a combination of both is seen in clinical practice. Cam impingement is a result of reduced anterior femoral head neck offset. Pincer lesion is caused by abnormalities on the acetabular side. FAI due to either mechanism can lead to chondral lesions and labral pathology. Patients present with groin pain and investigated with radiographs, CT and MRA. Surgery is the treatment of choice. Open or arthroscopic exploration of the hip is undertaken with bony resection to improve the femoral head neck junction with resection or repair of the damaged labrum. This may involve femoral osteochondroplasty for the cam lesion and acetabular rim resection for pincer lesion. There is no difference in outcome between open and arthroscopic surgery for FAI.
Keywords: Cam; Femoro-aecetabular; Hip; Impingement; Pincer; Young adults.
Figures


References
-
- Hossain M, Andrew JG. Current management of femoroacetabular impingement. Curr Orthop. 2008;22:300–310. doi: 10.1016/j.cuor.2008.07.011. - DOI
-
- Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Ortop. 2003;417:112–120. - PubMed
-
- Mayers SR, Eijer H, Ganz R. Anterior femoroacetabular impingement after periacetabular osteotomy. Clin Ortop. 1999;363:93–99. - PubMed
-
- Stulberg SD, Cordell LD, Harris WH, et al. Unrecognised childhood disease: a major cause of idiopathic osteoarthritis of the hip. The Proceedings of the Third Open Scientific Meeting of the Hip Society.St Louis, MO:CV Mosby;1975:212–2
LinkOut - more resources
Full Text Sources
Other Literature Sources
