

Wasting in chronic kidney disease
- PMID: 21475675
- PMCID: PMC3063874
- DOI: 10.1007/s13539-011-0019-5
Wasting in chronic kidney disease
Erratum in
-
Erratum to: Wasting in chronic kidney disease.J Cachexia Sarcopenia Muscle. 2011 Jun;2(2):119. doi: 10.1007/s13539-011-0026-6. J Cachexia Sarcopenia Muscle. 2011. PMID: 22477651 Free PMC article. No abstract available.
Abstract
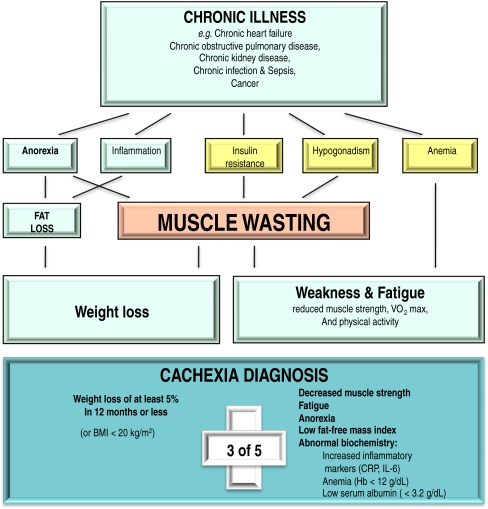
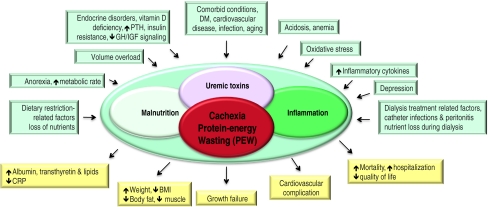
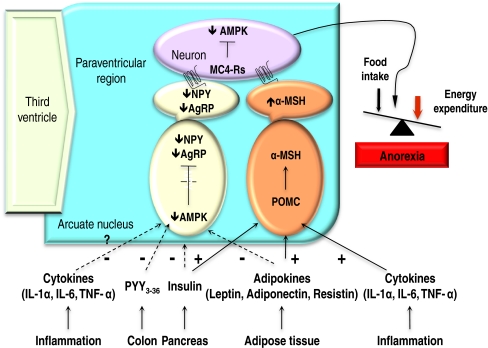
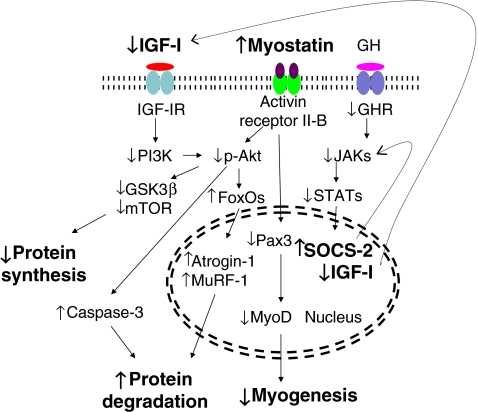
Wasting/cachexia is prevalent among patients with chronic kidney disease (CKD). It is to be distinguished from malnutrition, which is defined as the consequence of insufficient food intake or an improper diet. Malnutrition is characterized by hunger, which is an adaptive response, whereas anorexia is prevalent in patients with wasting/cachexia. Energy expenditure decreases as a protective mechanism in malnutrition whereas it remains inappropriately high in cachexia/wasting. In malnutrition, fat mass is preferentially lost and lean body mass and muscle mass is preserved. In cachexia/wasting, muscle is wasted and fat is relatively underutilized. Restoring adequate food intake or altering the composition of the diet reverses malnutrition. Nutrition supplementation does not totally reverse cachexia/wasting. The diagnostic criteria of cachexia/protein-energy wasting in CKD are considered. The association of wasting surrogates, such as serum albumin and prealbumin, with mortality is strong making them robust outcome predictors. At the patient level, longevity has consistently been observed in patients with CKD who have more muscle and/or fat, who report better appetite and who eat more. Although inadequate nutritional intake may contribute to wasting or cachexia, recent evidence indicates that other factors, including systemic inflammation, perturbations of appetite-controlling hormones from reduced renal clearance, aberrant neuropeptide signaling, insulin and insulin-like growth factor resistance, and metabolic acidosis, may be important in the pathogenesis of CKD-associated wasting. A number of novel therapeutic approaches, such as ghrelin agonists and melanocortin receptor antagonists are currently at the experimental level and await confirmation by randomized controlled clinical trials in patients with CKD-associated cachexia/wasting syndrome.
Figures
References
-
- Kopple JD. McCollum Award Lecture, 1996: protein–energy malnutrition in maintenance hemodialysis patients. Am J Clin Nutr. 1996;65:1544–1557. - PubMed
-
- Kalantar-Zadeh K, Ikizler TA, Block G, Avram MM, Kopple JD. Malnutrition–inflammation complex syndrome in dialysis patients: causes and consequence. Am J Kidney Dis. 2003;42:864–881. - PubMed
-
- World Health Organization. Wasting...stunting. World Health Organization. 1988; 10–3, May.
-
- Mak RH, Cheung W. Energy homeostasis and cachexia in chronic kidney disease. Pediatr Nephrol. 2006;21:1807–1814. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
