

Health related quality of life in trauma patients. Data from a one-year follow up study compared with the general population
- PMID: 21477280
- PMCID: PMC3088534
- DOI: 10.1186/1757-7241-19-22
Health related quality of life in trauma patients. Data from a one-year follow up study compared with the general population
Abstract
Background: Trauma patients have impaired health-related quality of life (HRQOL) after trauma. The aim of the study was to assess HRQOL during the first year after trauma and hospital stay in trauma patients admitted to an intensive-care unit (ICU) for >24 hours compared with non-ICU trauma patients and the general population, and to identify predictors of HRQOL.
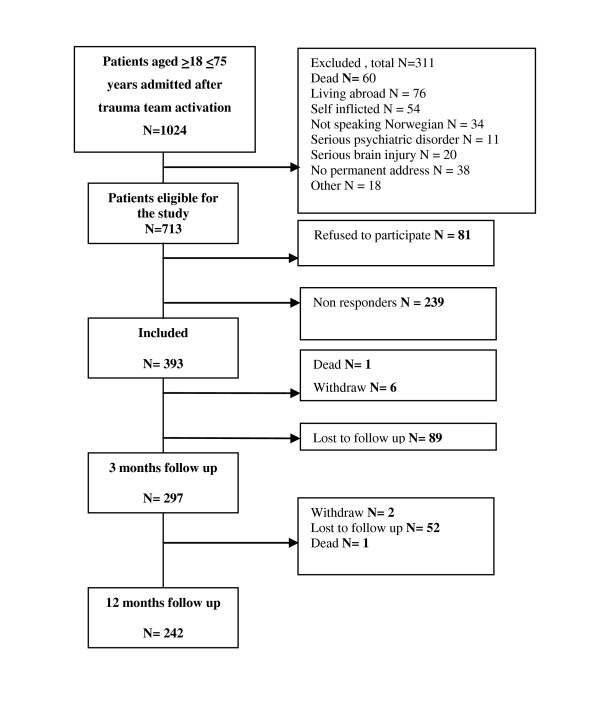
Methods: A prospective one-year follow-up study of 242 trauma patients received by the trauma team of a trauma referral centre in Norway was performed. HRQOL was measured using the Medical Outcomes Study Short Form 36 (SF-36) at 3 and 12 months.
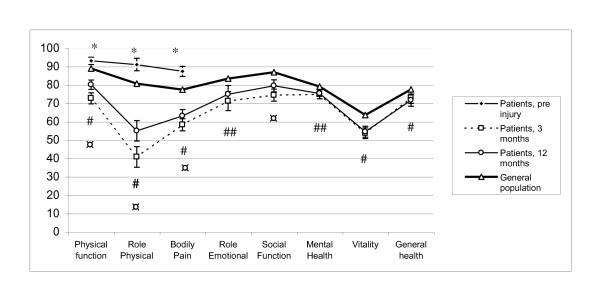
Results: The mean age of the cohort was 42.3 years (95% CI, 40.4-44.3 years). The median Injury Severity Score (ISS) was 10, interquartile range 16. The HRQOL improved significantly from the 3 to the 12 months follow up in the trauma patients. However their scores were significantly lower for most subscales of SF-36 compared to the general population. Significant differences between ICU and non-ICU patients at 12 months were observed only for physical functioning and role physical subscales. Optimism was an independent predictor of good HRQOL at 12 months, in all dimensions (beta, 0.95-2.45). A higher depression score at baseline predicted lower HRQOL in four of eight dimensions (beta -1.1 to -1.70). In addition, better physical functioning was predicted by lower age (beta, -0.20), and having head injury (reference) as the most severe injury vs. spine or extremity injuries (beta, -9.49 and -10.85), and better mental health by higher age (beta, 0.21) and being employed or studying before the trauma (beta, 12.27). In addition to optimism good general health was predicted by lower score for post-traumatic stress (PTS) symptoms at baseline (beta, -0.27) and lower ISS score (beta -10.59).
Conclusions: The HRQOL improved significantly from the 3 to the 12 months follow up in our sample. However their scores were significantly lower for most subscales of SF-36 compared to the general population. Significant differences between ICU and non-ICU patients were observed for only two subscales. Better HRQOL at 12 months was predicted mainly by optimism, low score for depression and PTS symptoms at baseline. High ISS predicted low general health exclusively.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
