

Stereotactic body radiation therapy for melanoma and renal cell carcinoma: impact of single fraction equivalent dose on local control
- PMID: 21477295
- PMCID: PMC3094365
- DOI: 10.1186/1748-717X-6-34
Stereotactic body radiation therapy for melanoma and renal cell carcinoma: impact of single fraction equivalent dose on local control
Abstract
Background: Melanoma and renal cell carcinoma (RCC) are traditionally considered less radioresponsive than other histologies. Whereas stereotactic body radiation therapy (SBRT) involves radiation dose intensification via escalation, we hypothesize SBRT might result in similar high local control rates as previously published on metastases of varying histologies.
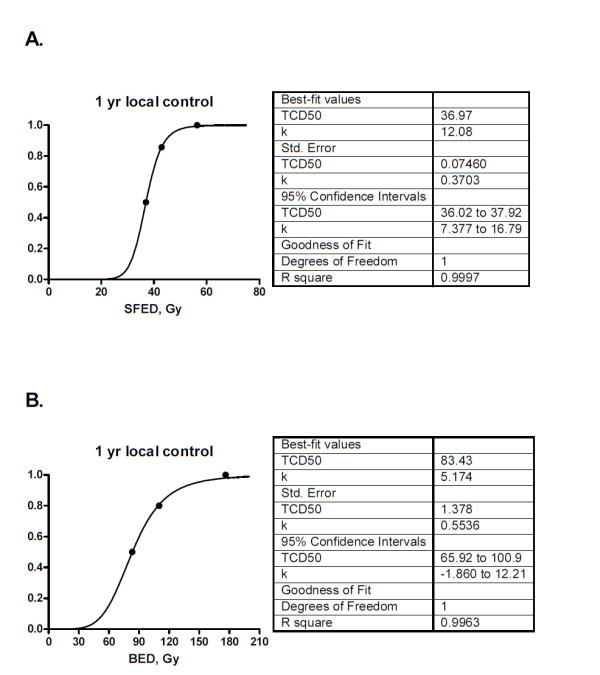
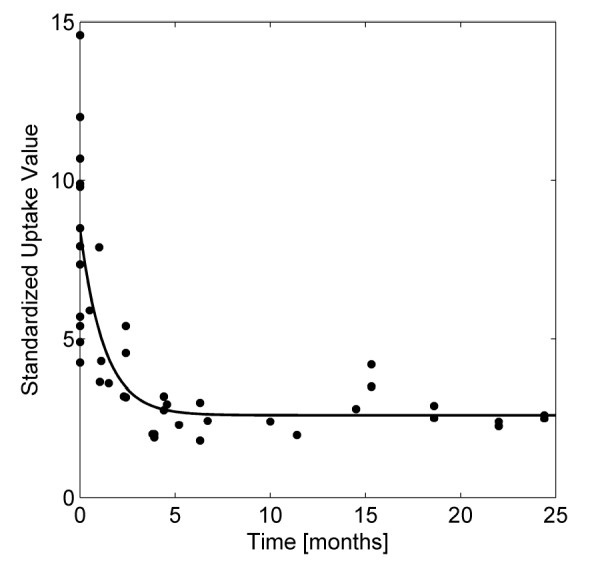
Methods: The records of patients with metastatic melanoma (n = 17 patients, 28 lesions) or RCC (n = 13 patients, 25 lesions) treated with SBRT were reviewed. Local control (LC) was defined pathologically by negative biopsy or radiographically by lack of tumor enlargement on CT or stable/declining standardized uptake value (SUV) on PET scan. The SBRT dose regimen was converted to the single fraction equivalent dose (SFED) to characterize the dose-control relationship using a logistic tumor control probability (TCP) model. Additionally, the kinetics of decline in maximum SUV (SUVmax) were analyzed.
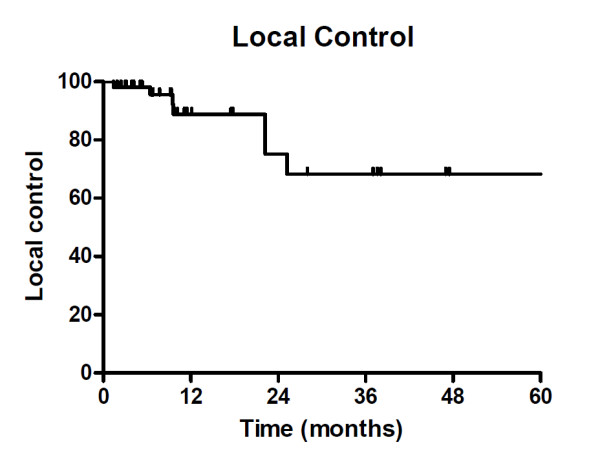
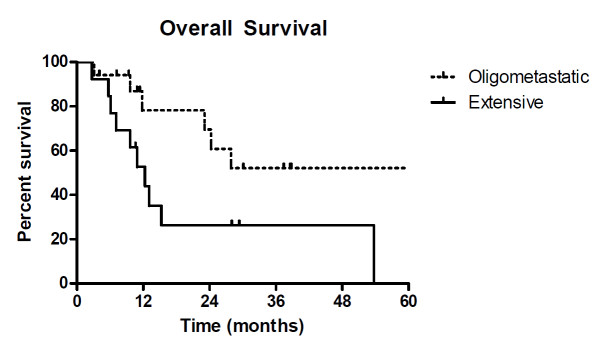
Results: The SBRT regimen was 40-50 Gy/5 fractions (n = 23) or 42-60 Gy/3 fractions (n = 30) delivered to lung (n = 39), liver (n = 11) and bone (n = 3) metastases. Median follow-up for patients alive at the time of analysis was 28.0 months (range, 4-68). The actuarial LC was 88% at 18 months. On univariate analysis, higher dose per fraction (p < 0.01) and higher SFED (p = 0.06) were correlated with better LC, as was the biologic effective dose (BED, p < 0.05). The actuarial rate of LC at 24 months was 100% for SFED ≥45 Gy v 54% for SFED <45 Gy. TCP modeling indicated that to achieve ≥90% 2 yr LC in a 3 fraction regimen, a prescription dose of at least 48 Gy is required. In 9 patients followed with PET scans, the mean pre-SBRT SUVmax was 7.9 and declined with an estimated half-life of 3.8 months to a post-treatment plateau of approximately 3.
Conclusions: An aggressive SBRT regimen with SFED ≥ 45 Gy is effective for controlling metastatic melanoma and RCC. The SFED metric appeared to be as robust as the BED in characterizing dose-response, though additional studies are needed. The LC rates achieved are comparable to those obtained with SBRT for other histologies, suggesting a dominant mechanism of in vivo tumor ablation that overrides intrinsic differences in cellular radiosensitivity between histologic subtypes.
Figures
Similar articles
-
Oligo metastatic renal cell carcinoma: stereotactic body radiation therapy, if, when and how?Clin Transl Oncol. 2021 Aug;23(8):1717-1726. doi: 10.1007/s12094-021-02574-0. Epub 2021 Mar 9. Clin Transl Oncol. 2021. PMID: 33687659
-
Local Control Rates of Metastatic Renal Cell Carcinoma (RCC) to Thoracic, Abdominal, and Soft Tissue Lesions Using Stereotactic Body Radiotherapy (SBRT).Radiat Oncol. 2015 Oct 28;10:218. doi: 10.1186/s13014-015-0528-z. Radiat Oncol. 2015. PMID: 26510665 Free PMC article.
-
Single-fraction versus multifraction spinal stereotactic radiosurgery for spinal metastases from renal cell carcinoma: secondary analysis of Phase I/II trials.J Neurosurg Spine. 2016 May;24(5):829-36. doi: 10.3171/2015.8.SPINE15844. Epub 2016 Jan 22. J Neurosurg Spine. 2016. PMID: 26799117 Clinical Trial.
-
Tumor Control Probability Modeling and Systematic Review of the Literature of Stereotactic Body Radiation Therapy for Prostate Cancer.Int J Radiat Oncol Biol Phys. 2021 May 1;110(1):227-236. doi: 10.1016/j.ijrobp.2020.08.014. Epub 2020 Sep 6. Int J Radiat Oncol Biol Phys. 2021. PMID: 32900561 Free PMC article.
-
When Surgery Is Not an Option in Renal Cell Carcinoma: The Evolving Role of Stereotactic Body Radiation Therapy.Oncology (Williston Park). 2019 May 14;33(5):167-73, 177. Oncology (Williston Park). 2019. PMID: 31095714 Review.
Cited by
-
Clinical outcomes of cyberknife stereotactic radiosurgery for lung metastases.J Thorac Dis. 2015 Mar;7(3):407-12. doi: 10.3978/j.issn.2072-1439.2015.01.09. J Thorac Dis. 2015. PMID: 25922719 Free PMC article.
-
Local control rates of metastatic renal cell carcinoma (RCC) to the bone using stereotactic body radiation therapy: Is RCC truly radioresistant?Pract Radiat Oncol. 2015 Nov-Dec;5(6):e589-e596. doi: 10.1016/j.prro.2015.05.004. Epub 2015 Jun 30. Pract Radiat Oncol. 2015. PMID: 26142027 Free PMC article.
-
The Efficacy of Conventionally Fractionated Radiation in the Management of Osseous Metastases from Metastatic Renal Cell Carcinoma.J Oncol. 2018 Jan 9;2018:6384253. doi: 10.1155/2018/6384253. eCollection 2018. J Oncol. 2018. PMID: 29552034 Free PMC article.
-
Radiation-induced autophagy potentiates immunotherapy of cancer via up-regulation of mannose 6-phosphate receptor on tumor cells in mice.Cancer Immunol Immunother. 2014 Oct;63(10):1009-21. doi: 10.1007/s00262-014-1573-4. Epub 2014 Jun 19. Cancer Immunol Immunother. 2014. PMID: 24943275 Free PMC article.
-
Novel application of stereotactic ablative radiotherapy using CyberKnife® for early-stage renal cell carcinoma in patients with pre-existing chronic kidney disease: Initial clinical experiences.Oncol Lett. 2014 Jul;8(1):355-360. doi: 10.3892/ol.2014.2129. Epub 2014 May 9. Oncol Lett. 2014. PMID: 24959276 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
