

Myocardial infarction (ST-elevation)
- PMID: 21477402
- PMCID: PMC3217814
Myocardial infarction (ST-elevation)
Abstract
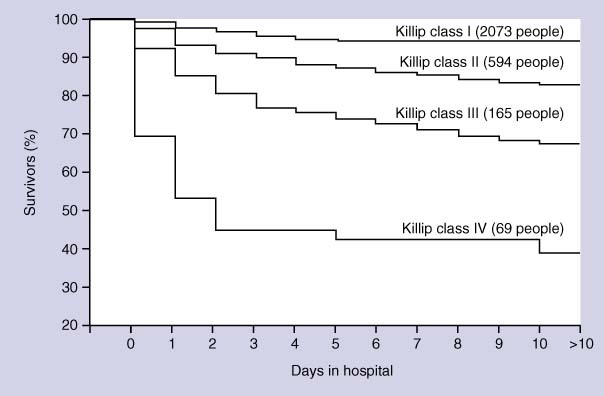
Introduction: About one quarter of people having an acute myocardial infarction (MI) in the USA will die of it, half of them within 1 hour of the onset of symptoms. Cardiogenic shock develops in over 5% of people surviving the first hour after an acute MI, with a mortality of 50% to 80% in the first 48 hours.
Methods and outcomes: We conducted a systematic review and aimed to answer the following clinical questions: Which treatments improve outcomes in acute MI? Which treatments improve outcomes for cardiogenic shock after MI? We searched: Medline, Embase, The Cochrane Library, and other important databases up to October 2009 (Clinical Evidence reviews are updated periodically, please check our website for the most up-to-date version of this review). We included harms alerts from relevant organisations such as the US Food and Drug Administration (FDA) and the UK Medicines and Healthcare products Regulatory Agency (MHRA).
Results: We found 52 systematic reviews, RCTs, or observational studies that met our inclusion criteria. We performed a GRADE evaluation of the quality of evidence for interventions.
Conclusions: In this systematic review we present information relating to the effectiveness and safety of the following interventions: angiotensin-converting enzyme (ACE) inhibitors, aspirin, beta-blockers, calcium channel blockers, early cardiac surgery, early invasive cardiac revascularisation, glycoprotein IIb/IIIa inhibitors, intra-aortic balloon counterpulsation, nitrates (with or without thrombolysis), positive inotropes, primary percutaneous transluminal coronary angioplasty (PTCA), pulmonary artery catheterisation, thrombolysis (with or without low molecular weight heparin, with or without unfractionated heparin), vasodilators, and ventricular assistance devices and cardiac transplantation.
Figures
Similar articles
-
Myocardial infarction (ST-elevation).BMJ Clin Evid. 2009 Jan 9;2009:0202. BMJ Clin Evid. 2009. PMID: 19445779 Free PMC article.
-
Acute coronary syndrome (unstable angina and non-ST elevation MI).BMJ Clin Evid. 2009 Jan 13;2009:0209. BMJ Clin Evid. 2009. PMID: 19445778 Free PMC article.
-
Secondary prevention of ischaemic cardiac events.BMJ Clin Evid. 2011 Aug 30;2011:0206. BMJ Clin Evid. 2011. PMID: 21875445 Free PMC article.
-
Non ST-elevation acute coronary syndrome.BMJ Clin Evid. 2010 Nov 15;2010:0209. BMJ Clin Evid. 2010. PMID: 21406132 Free PMC article.
-
Routine invasive strategies versus selective invasive strategies for unstable angina and non-ST elevation myocardial infarction in the stent era.Cochrane Database Syst Rev. 2016 May 26;2016(5):CD004815. doi: 10.1002/14651858.CD004815.pub4. Cochrane Database Syst Rev. 2016. PMID: 27226069 Free PMC article.
Cited by
-
Add-on effect of chinese herbal medicine on mortality in myocardial infarction: systematic review and meta-analysis of randomized controlled trials.Evid Based Complement Alternat Med. 2013;2013:675906. doi: 10.1155/2013/675906. Epub 2013 Jan 10. Evid Based Complement Alternat Med. 2013. PMID: 23365612 Free PMC article.
References
-
- Califf RM, Bengtson JR. Cardiogenic shock. N Engl J Med 1994;330:1724–1730. - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, et al, for the SHOCK investigators. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med 1999;341:625–634. - PubMed
-
- Urban P, Stauffer JC, Khatchatrian N, et al. A randomized evaluation of early revascularization to treat shock complicating acute myocardial infarction. The (Swiss) Multicenter Trial of Angioplasty for Shock — (S)MASH. Eur Heart J 1999;20:1030–1038. - PubMed
-
- Murray C, Lopez A. Mortality by cause for eight regions of the world: global burden of disease study. Lancet 1997;349:1269–1276. - PubMed
-
- National Heart, Lung, and Blood Institute. Morbidity and mortality: chartbook on cardiovascular, lung, and blood diseases. Bethesda, MD: US Department of Health and Human Services, Public Health Service, National Institutes of Health; May 1992.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous