

Spontaneous emergence of multiple drug resistance in tuberculosis before and during therapy
- PMID: 21479171
- PMCID: PMC3068161
- DOI: 10.1371/journal.pone.0018327
Spontaneous emergence of multiple drug resistance in tuberculosis before and during therapy
Abstract
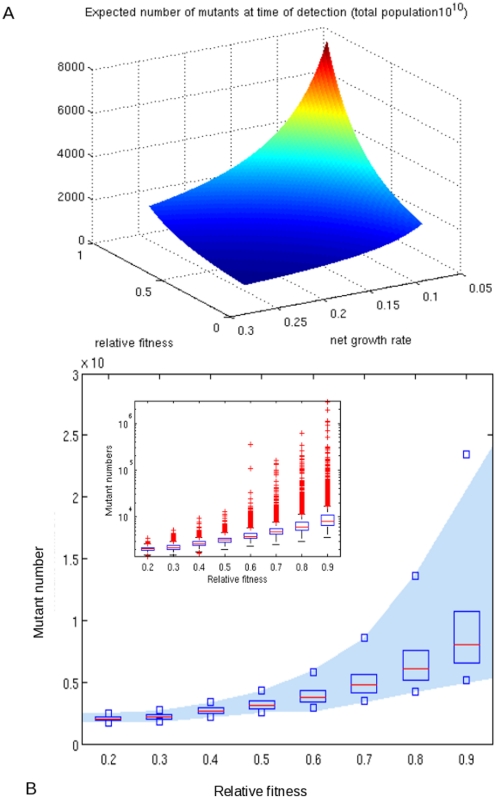
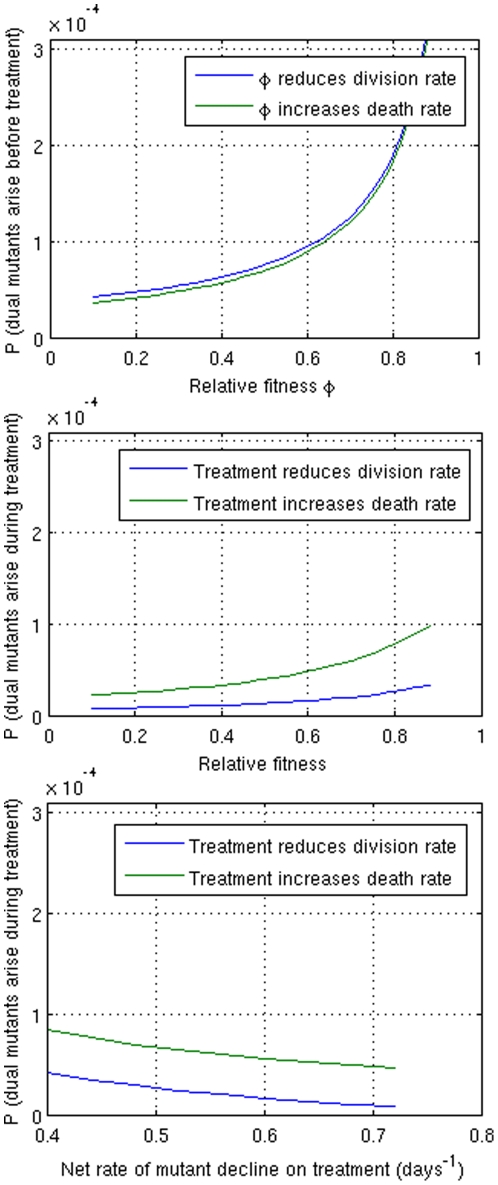
The emergence of drug resistance in M. tuberculosis undermines the efficacy of tuberculosis (TB) treatment in individuals and of TB control programs in populations. Multiple drug resistance is often attributed to sequential functional monotherapy, and standard initial treatment regimens have therefore been designed to include simultaneous use of four different antibiotics. Despite the widespread use of combination therapy, highly resistant M. tb strains have emerged in many settings. Here we use a stochastic birth-death model to estimate the probability of the emergence of multidrug resistance during the growth of a population of initially drug sensitive TB bacilli within an infected host. We find that the probability of the emergence of resistance to the two principal anti-TB drugs before initiation of therapy ranges from 10(-5) to 10(-4); while rare, this is several orders of magnitude higher than previous estimates. This finding suggests that multidrug resistant M. tb may not be an entirely "man-made" phenomenon and may help explain how highly drug resistant forms of TB have independently emerged in many settings.
Conflict of interest statement
Figures
References
-
- The Stop TB Department World Health Organization. Countries that had reported at least one XDR-TB case by September 2009. WHO 2009.
-
- Perdigão J, Macedo R, Malaquias A, Ferreira A, Brum L, Portugal L. Genetic analysis of extensively drug-resistant Mycobacterium tuberculosis strains in Lisbon, Portugal. J Antimicrob Chemother. 2010;65:224–227. - PubMed
-
- Mlambo M, Warren RM, Poswa X, Victor TC, Duse AG, Marais E. Genotypic diversity of extensively drug-resistant tuberculosis (XDR-TB) in South Africa. Int J Tuberc Lung Dis. 2008;12:99–104. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
