

High resolution imaging of tunnels by magnetic resonance neurography
- PMID: 21479520
- PMCID: PMC3158963
- DOI: 10.1007/s00256-011-1143-1
High resolution imaging of tunnels by magnetic resonance neurography
Abstract
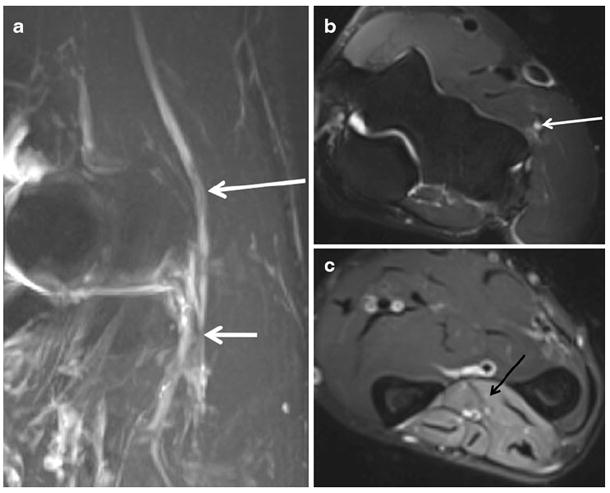
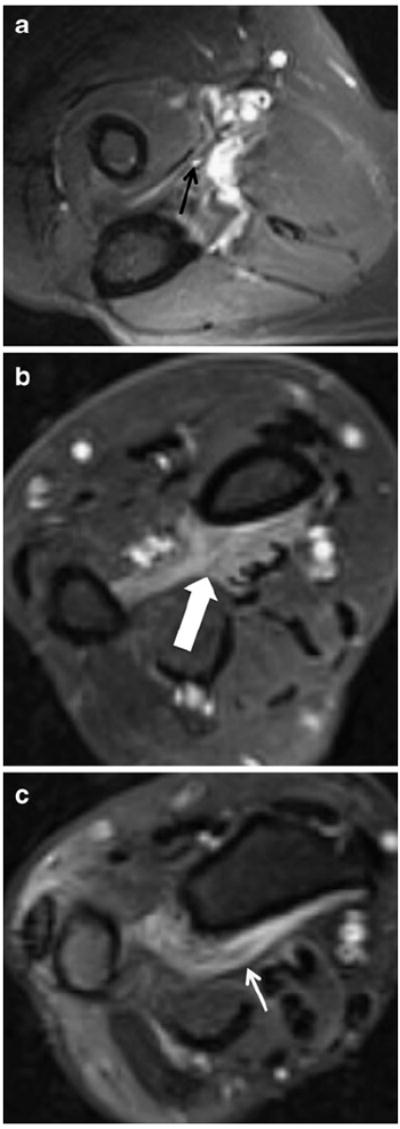
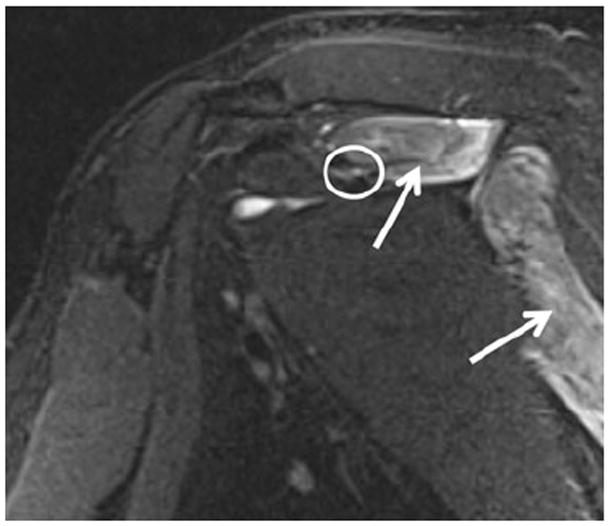
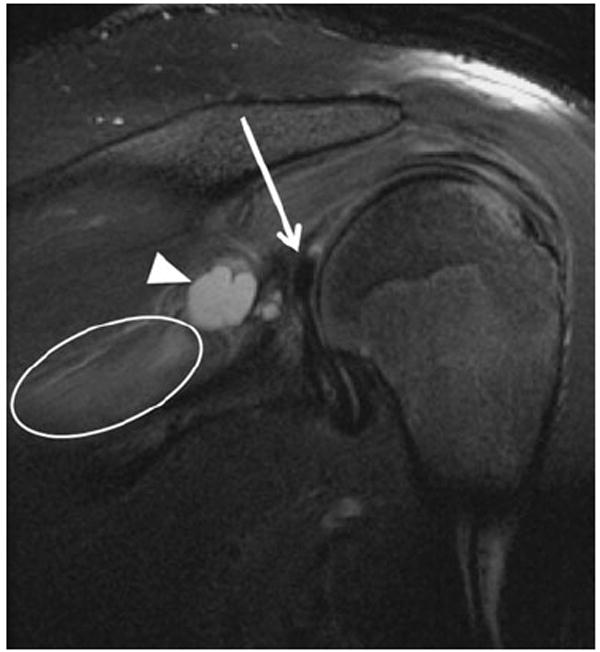
Peripheral nerves often traverse confined fibro-osseous and fibro-muscular tunnels in the extremities, where they are particularly vulnerable to entrapment and compressive neuropathy. This gives rise to various tunnel syndromes, characterized by distinct patterns of muscular weakness and sensory deficits. This article focuses on several upper and lower extremity tunnels, in which direct visualization of the normal and abnormal nerve in question is possible with high resolution 3T MR neurography (MRN). MRN can also serve as a useful adjunct to clinical and electrophysiologic exams by discriminating adhesive lesions (perineural scar) from compressive lesions (such as tumor, ganglion, hypertrophic callous, or anomalous muscles) responsible for symptoms, thereby guiding appropriate treatment.
Conflict of interest statement
Figures
Similar articles
-
High-resolution magnetic resonance neurography in upper extremity neuropathy.Neuroimaging Clin N Am. 2014 Feb;24(1):109-25. doi: 10.1016/j.nic.2013.03.025. Epub 2013 May 30. Neuroimaging Clin N Am. 2014. PMID: 24210316 Review.
-
MR Neurography: Diagnostic Imaging in the PNS.Clin Neuroradiol. 2015 Oct;25 Suppl 2:283-9. doi: 10.1007/s00062-015-0412-0. Epub 2015 Jun 13. Clin Neuroradiol. 2015. PMID: 26070607
-
MR imaging mapping of skeletal muscle denervation in entrapment and compressive neuropathies.Radiographics. 2011 Mar-Apr;31(2):319-32. doi: 10.1148/rg.312105122. Radiographics. 2011. PMID: 21415181 Review.
-
Peripheral MR neurography: approach to interpretation.Neuroimaging Clin N Am. 2014 Feb;24(1):79-89. doi: 10.1016/j.nic.2013.03.033. Epub 2013 May 25. Neuroimaging Clin N Am. 2014. PMID: 24210314 Review.
-
MRI of sports-related peripheral nerve injuries.AJR Am J Roentgenol. 2014 Nov;203(5):1075-84. doi: 10.2214/AJR.13.12183. AJR Am J Roentgenol. 2014. PMID: 25341148 Review.
Cited by
-
Glossary of terms for musculoskeletal radiology.Skeletal Radiol. 2020 Jul;49(Suppl 1):1-33. doi: 10.1007/s00256-020-03465-1. Epub 2020 Jun 2. Skeletal Radiol. 2020. PMID: 32488336 Free PMC article. Review.
-
Impact of high resolution 3 tesla MR neurography (MRN) on diagnostic thinking and therapeutic patient management.Eur Radiol. 2016 May;26(5):1235-44. doi: 10.1007/s00330-015-3958-y. Epub 2015 Sep 22. Eur Radiol. 2016. PMID: 26396110
-
MR imaging of the postsurgical cubital tunnel: an imaging review of the cubital tunnel, cubital tunnel syndrome, and associated surgical techniques.Skeletal Radiol. 2019 Oct;48(10):1541-1554. doi: 10.1007/s00256-019-03203-2. Epub 2019 Mar 28. Skeletal Radiol. 2019. PMID: 30919024 Review.
-
T2-signal of ulnar nerve branches at the wrist in guyon's canal syndrome.PLoS One. 2012;7(10):e47295. doi: 10.1371/journal.pone.0047295. Epub 2012 Oct 10. PLoS One. 2012. PMID: 23071777 Free PMC article.
-
MRI grading using the neuropathy score-reporting and data system with electrodiagnostic correlation in radial neuropathy around the elbow: a 13-year retrospective review.Skeletal Radiol. 2025 Aug;54(8):1621-1630. doi: 10.1007/s00256-024-04861-7. Epub 2025 Jan 6. Skeletal Radiol. 2025. PMID: 39760931
References
-
- Siemionow M, Brzezicki G. Chapter 8: current techniques and concepts in peripheral nerve repair. Int Rev Neurobiol. 2009;87:141–72. - PubMed
-
- Pećina M, Krmpotić-Nemanić J, Markiewitz AD. Tunnel syndromes. 3. Boca Raton: CRC Press; 2001.
-
- Gutmann L. Pearls and pitfalls in the use of electromyography and nerve conduction studies. Semin Neurol. 2003;23:77–82. - PubMed
-
- Bashir WA, Connell DA. Imaging of entrapment and compressive neuropathies. Semin Musculoskelet Radiol. 2008;12:170–81. - PubMed
-
- Spratt JD, Stanley AJ, Grainger AJ, Hide IG, Campbell RSD. The role of diagnostic radiology in compressive and entrapment neuropathies. Eur Radiol. 2002;12:2352–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
