

Associations between salivary gland histopathologic diagnoses and phenotypic features of Sjögren's syndrome among 1,726 registry participants
- PMID: 21480190
- PMCID: PMC3128201
- DOI: 10.1002/art.30381
Associations between salivary gland histopathologic diagnoses and phenotypic features of Sjögren's syndrome among 1,726 registry participants
Abstract
Objective: To examine associations between labial salivary gland (LSG) histopathology and other phenotypic features of Sjögren's syndrome (SS).
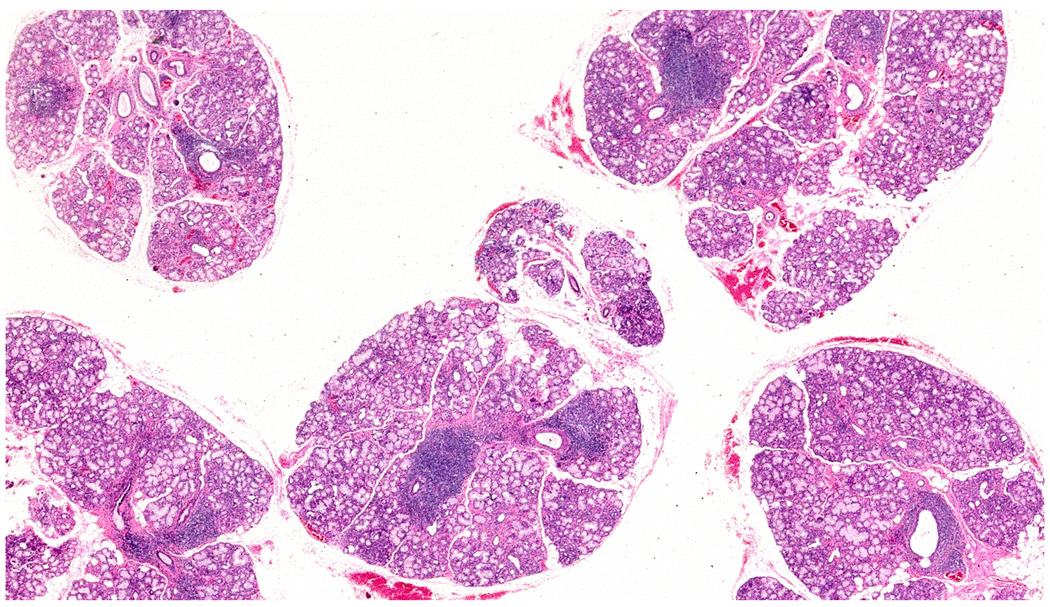
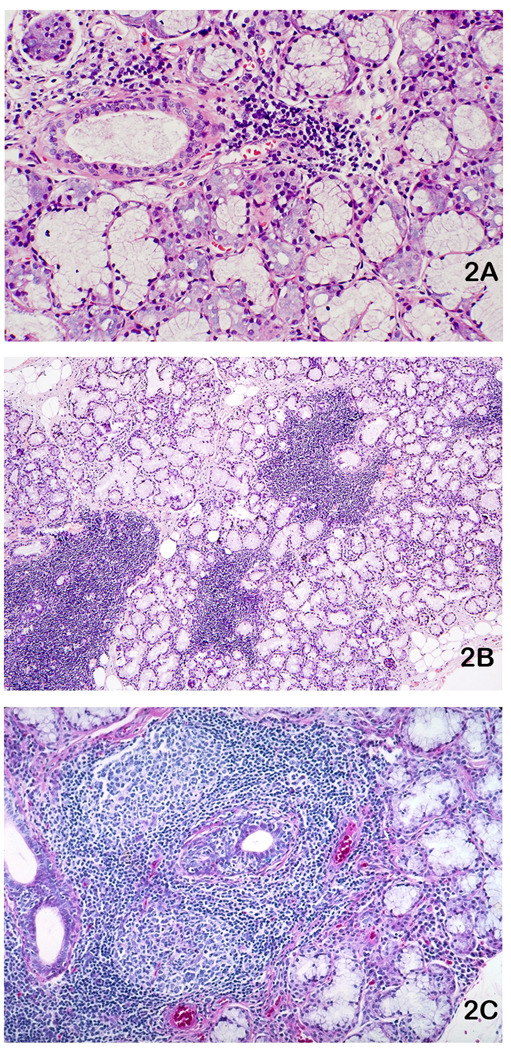
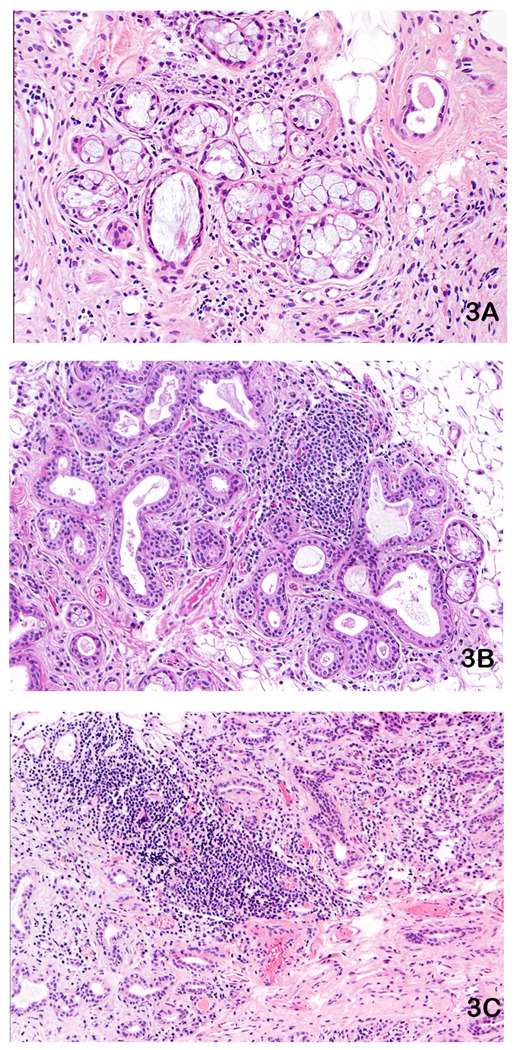
Methods: The database of the Sjögren's International Collaborative Clinical Alliance (SICCA), a registry of patients with symptoms of possible SS as well as those with obvious disease, was used for the present study. LSG biopsy specimens from SICCA participants were subjected to protocol-directed histopathologic assessments. Among the 1,726 LSG specimens exhibiting any pattern of sialadenitis, we compared biopsy diagnoses against concurrent salivary, ocular, and serologic features.
Results: LSG specimens included 61% with focal lymphocytic sialadenitis (FLS; 69% of which had focus scores of ≥1 per 4 mm²) and 37% with nonspecific or sclerosing chronic sialadenitis (NS/SCS). Focus scores of ≥1 were strongly associated with serum anti-SSA/SSB positivity, rheumatoid factor, and the ocular component of SS, but not with symptoms of dry mouth or dry eyes. Those with positive anti-SSA/SSB were 9 times (95% confidence interval [95% CI] 7.4-11.9) more likely to have a focus score of ≥1 than were those without anti-SSA/SSB, and those with an unstimulated whole salivary flow rate of <0.1 ml/minute were 2 times (95% CI 1.7-2.8) more likely to have a focus score of ≥1 than were those with a higher flow rate, after controlling for other phenotypic features of SS.
Conclusion: Distinguishing FLS from NS/SCS is essential in assessing LSG biopsies, before determining focus score. A diagnosis of FLS with a focus score of ≥1 per 4 mm², as compared to FLS with a focus score of <1 or NS/SCS, is strongly associated with the ocular and serologic components of SS and reflects SS autoimmunity.
Copyright © 2011 by the American College of Rheumatology.
Figures
References
-
- Sjögren H. Zur kenntnis der keratoconjunctivitis sicca (Keratitis filiformis bei Hypofunktion der Tränendrüsen) Acta Ophthalmol (Copenh) 1933;11 Suppl 2:1–151. English translation by JB Hamilton: Sjögren H. A New Conception of Keratoconjunctivitis Sicca. Sydney, Australasian Medical Publishing Co. Ltd., 1943.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
